
The Myth That Has Kept Women Away From the Most Important Exercise They Could Be Doing
Women weight training benefits is a subject worth communicating clearly, because the single biggest obstacle standing between most women and the most effective exercise available to them is a misconception so deeply embedded it has taken on the quality of received wisdom. The fear that lifting weights will make a woman bulky, masculine, or disproportionately muscular has steered generations of women toward treadmills, step classes, and low-resistance circuits that produce a fraction of the health and body composition benefits that resistance training delivers.
I understand where the fear comes from. The images associated with female weightlifting in popular culture have historically been extreme: competitive bodybuilders and powerlifters whose physiques represent years of highly specialised training, specific dietary strategies, and in many cases pharmaceutical assistance. These are not the outcomes of three resistance sessions per week with progressive loading. They are the outcomes of a very specific and deliberately pursued training protocol that most women are not following and have no intention of following.
The reality of what happens to a woman's body when she commits to an intelligently designed resistance training programme is this: she becomes leaner, stronger, more energetic, more metabolically resilient, and in the vast majority of cases, significantly happier with how she looks and feels. The word bulky does not enter the picture. The word transformation does.
This article gives you the biology, the evidence, and the practical framework to understand why weight training is the most important exercise a woman can do, and how to approach it in a way that produces the results you actually want.
The Testosterone Reality: Why Women Cannot Accidentally Become Bulky
The fear of becoming bulky from lifting weights is fundamentally a misunderstanding of the hormonal conditions required to build significant muscle mass. Building the kind of muscular development that most women want to avoid requires a combination of factors that the female body simply does not produce naturally.
Testosterone is the primary anabolic hormone driving muscle hypertrophy. Men produce testosterone in the range of 270 to 1,070 nanograms per decilitre. Women produce testosterone in the range of 15 to 70 nanograms per decilitre. That is a difference of approximately fifteen to twenty times. This is not a small hormonal variation. It is a categorical biological distinction that fundamentally limits the degree of muscle hypertrophy a woman can achieve through natural training (1).
Oestrogen, the dominant sex hormone in premenopausal women, has a moderating effect on muscle hypertrophy. While it supports muscle protein synthesis and recovery, its presence alongside low testosterone creates a hormonal environment that favours a leaner, more defined physique over the kind of significant muscle bulk that requires high testosterone to sustain. Women who train consistently with weights develop muscle tone and definition. They do not, in the absence of pharmaceutical intervention, develop the muscle mass that characterises competitive male bodybuilders.
The women who appear significantly muscular in media and fitness contexts have in the majority of cases been training for many years with exceptional consistency and precision, following very specific high-volume hypertrophy protocols, managing nutrition to a high degree of precision, and in competitive contexts, often using anabolic substances. None of this happens accidentally or as an unintended consequence of a few resistance training sessions per week.
For the woman reading this who is concerned about becoming too muscular: the amount of deliberate, sustained effort required to build significant muscle mass is so substantial that the risk of doing so accidentally is, in practical terms, zero. The more realistic risk is the opposite: not doing enough resistance training and missing the metabolic, hormonal, and structural benefits it provides.
Top Tip
If you are new to resistance training or have been avoiding it out of concern about bulking, commit to three sessions per week for three months with progressive loading. Take a photograph at the start and after twelve weeks. The result, for virtually every woman who does this, is a leaner and more defined physique with the same or very similar body weight on the scale. The composition changes. The bulk does not arrive.
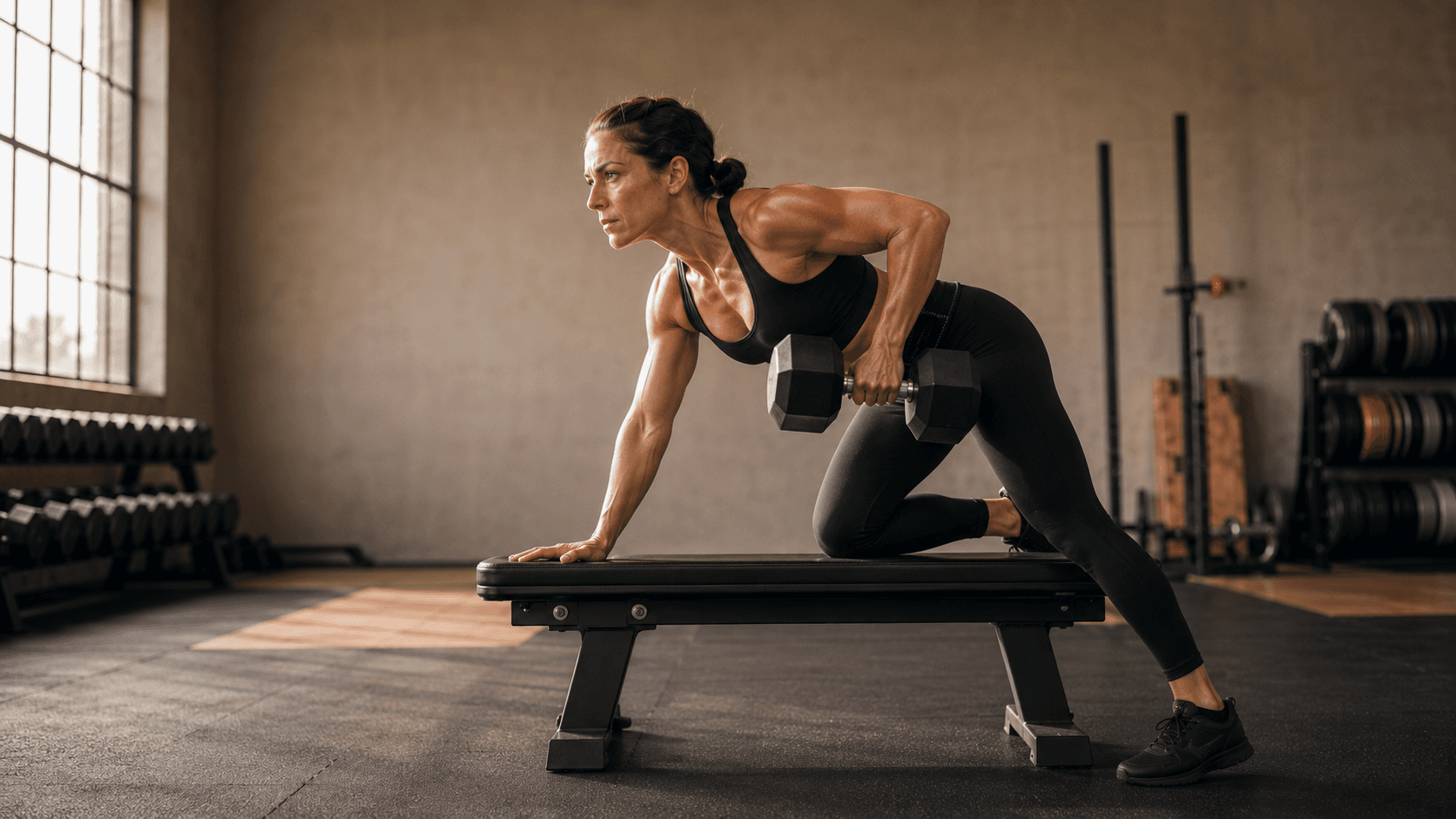
What Resistance Training Actually Does to a Woman's Body
Understanding what resistance training produces in the female body is the most effective antidote to the fear of it. These are not theoretical benefits. They are measurable, documented physiological outcomes supported by substantial research.
INPUT: Progressive resistance training · 3–4 sessions per week · Compound movements · Adequate protein
01
Body Composition
Replaces fat with lean muscle. Waist reduces. Shape improves. Scale weight may stay similar but body changes profoundly.
02
Metabolic Rate
Muscle tissue burns more energy at rest than fat tissue. Resting metabolic rate rises. Fat loss becomes easier and more sustainable over time.
03
Bone Density
Mechanical loading stimulates bone formation. The most evidence-supported intervention for preventing osteoporosis across the female lifespan.
04
Insulin Sensitivity
Muscle is the largest insulin-sensitive tissue in the body. More muscle means better blood glucose management. Type 2 diabetes and PCOS risk both reduced.
05
Hormonal Balance
Reduces cortisol chronically. Improves oestrogen metabolism. Reduces visceral fat that drives androgen excess. Supports thyroid function.
06
Cardiovascular Health
Lowers resting blood pressure. Improves lipid profile. Reduces inflammatory markers. Protects the heart and vascular system.
07
Mental Health
Consistent evidence for reductions in depression and anxiety. Improves self-efficacy and body image. Neurobiological mechanism via BDNF and endorphins.
08
Longevity and Function
Preserves physical capability into older age. Reduces falls risk. Maintains independence. The most important investment a woman can make in her future self.
09
Sleep Quality
Regular resistance training improves sleep onset, duration, and deep sleep quality. Supports the hormonal recovery that happens during sleep.
OUTPUT: A leaner, stronger, more metabolically resilient body with better hormones, better sleep, better mood, and significantly lower long-term disease risk. Not bulky. Better.
Cardio vs Resistance Training for Women: An Honest Comparison
Most women have been conditioned to see cardio as the primary fat loss tool and resistance training as something optional, secondary, or for a different kind of goal. The evidence does not support this hierarchy. The following comparison explains the distinction plainly.
| Health Outcome | Cardio Training Alone | Resistance Training (or Combination) |
|---|---|---|
| Fat loss | Burns calories during the session. Minimal effect on resting metabolic rate. Fat loss slows as the body adapts and becomes more efficient. | Burns fewer calories per session but raises resting metabolic rate through muscle gain. Fat loss effect compounds over time and remains effective as the body adapts. |
| Muscle preservation | High-volume cardio in a calorie deficit can cause muscle loss, which slows metabolic rate and worsens body composition over time. | Preserves and builds muscle tissue even in a modest calorie deficit. Protects metabolic rate during fat loss. |
| Bone density | Low-impact cardio has minimal effect on bone density. High-impact options like running have some benefit but carry injury risk. | Mechanical loading from resistance training is the most evidence-supported intervention for building and preserving bone density in women across all age groups. |
| Insulin sensitivity | Moderate benefit. Cardiovascular exercise improves insulin sensitivity acutely during and after exercise. | Building muscle mass creates a structural, permanent improvement in insulin sensitivity that persists even on rest days. The largest glucose-absorbing tissue in the body is skeletal muscle. |
| Hormonal impact | Excessive cardio volume elevates cortisol chronically and can suppress reproductive hormones in women, particularly in a calorie deficit. | Moderate resistance training improves hormonal balance: reduces cortisol chronically, supports oestrogen metabolism, improves thyroid function. |
| Cardiovascular health | Strong direct benefit for cardiovascular fitness, VO2 max, and cardiac output. Walking and moderate cardio are valuable for this purpose. | Also improves cardiovascular markers including blood pressure, lipid profile, and inflammation. Combines effectively with cardio for comprehensive heart health. |
| Metabolic rate long-term | Does not raise resting metabolic rate. Metabolic rate can decrease as cardio volume increases due to the body's efficiency adaptations. | Raises resting metabolic rate directly through increased muscle mass. The more muscle tissue a woman carries, the more energy she burns at rest, permanently. |
The evidence does not position cardio and resistance training as competitors. A combination of both produces the best overall health profile. The point is that resistance training should be the foundation of a woman's exercise programme, not an optional extra. Cardio complements it.
What Years of Cardio Without Resistance Training Actually Produces
I am going to be direct here because I think this is one of the most important things I can tell a woman who has spent years doing primarily cardio-based exercise and wondering why her body has not changed the way she hoped.
Sarcopenic obesity is a condition increasingly seen in women in their 40s and 50s who have spent years in a calorie deficit doing large amounts of cardio. It describes a body composition characterised by low muscle mass alongside excess body fat, often at a relatively normal total body weight. The scale looks acceptable. The metabolic picture does not. A woman with sarcopenic obesity has a slower metabolic rate, poorer insulin sensitivity, higher cardiovascular risk, lower bone density, and a body that is increasingly resistant to fat loss, precisely because the muscle tissue needed to drive metabolic rate and glucose clearance has never been built or has been lost through undereating and cardio without resistance training (2).
This is the destination that the combination of chronic restriction and cardio-dominant training points toward. Not rapidly or dramatically in most cases, but progressively and consistently. Each decade that passes without resistance training is a decade in which muscle mass is lost, bone density declines, metabolic rate falls, and the effort required to maintain the same body weight increases.
The women who come to me in their 40s and 50s having done all the right things, diet-wise and cardio-wise, and cannot understand why their body is changing in ways they do not want, are in most cases experiencing the cumulative consequence of under-prioritising resistance training for decades. The good news is that the response to resistance training remains robust across every age group. It is never too late to start. But the earlier a woman begins, the more she accumulates.
Top Tip
If you have been doing primarily cardio-based exercise for several years and your body composition has not changed significantly despite your efforts, or if you find that maintaining your current weight requires increasing amounts of exercise and decreasing amounts of food, muscle loss is likely a significant contributing factor. A structured resistance training programme is the most direct route to reversing this trajectory.

How to Structure a Resistance Training Programme for a Woman New to Lifting
The principles of effective resistance training for women are not complicated, but they require some clarity on what actually matters and what can be safely set aside.
Frequency: three to four sessions per week is the evidence-supported frequency for meaningful body composition and strength improvements in women. This is achievable within a busy schedule when sessions are structured efficiently. Each session should be forty-five to sixty minutes of purposeful work.
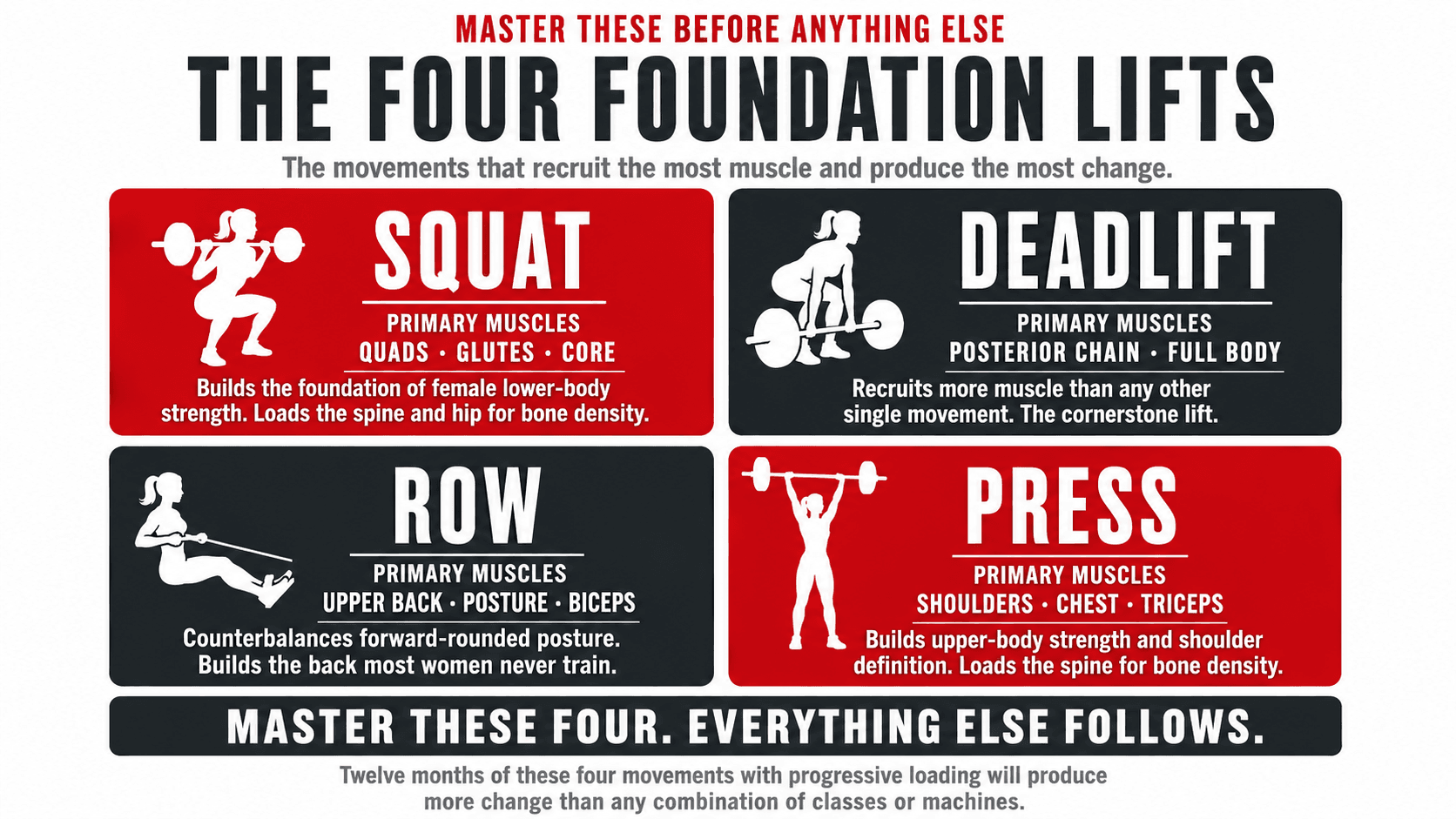
Exercise selection: compound movements that recruit multiple muscle groups simultaneously should form the foundation of every session. Squats, deadlifts, Romanian deadlifts, hip thrusts, rows, overhead press, and chest press recruit the largest volumes of muscle tissue and produce the greatest metabolic and structural stimulus. Isolation exercises, such as bicep curls and tricep extensions, have their place but should be additions to a compound foundation, not replacements for it.
Progressive overload: this is the mechanism through which training produces ongoing results. It means gradually increasing the stimulus over time, either by adding weight, adding repetitions, adding sets, or reducing rest periods. A woman who lifts the same weights for the same repetitions in every session for a year will not continue to make progress after the initial adaptation phase. The body adapts to the stimulus it receives and requires a progressively greater stimulus to continue adapting (3).
Effort level: the most common reason women do not get the results they want from resistance training is insufficient effort. Working with weights that allow thirty repetitions without meaningful effort produces a very different stimulus than working with weights where the final two to three repetitions of a set of eight to twelve require genuine exertion. The latter drives adaptation. The former produces maintenance at best. Training close to the point where another repetition would not be achievable with good form, typically leaving one to three repetitions in reserve, is the intensity required for meaningful progress.
Top Tip
Start with the four movements that recruit the most muscle tissue in the female body: the squat, the deadlift or Romanian deadlift, the row, and the press. Master the technique of each before adding significant load. These four movements alone, performed consistently with progressive loading for twelve months, will produce more meaningful body composition change than any combination of cardio-based classes or isolation machine work.
A Starting Framework for Women New to Resistance Training
The programme below is a practical starting point for a woman who is new to resistance training or who is returning after a significant break. It is not a definitive or permanent programme. It is a foundation from which to build.
| Session | Focus | Primary Movements | Supporting Work | Sets x Reps |
|---|---|---|---|---|
| Session A | Lower body: quad and glute dominant | Goblet squat or barbell squat. Romanian deadlift. Hip thrust. | Leg press. Walking lunges. Calf raises. | 3 to 4 sets of 8 to 12 reps |
| Session B | Upper body: push and pull | Dumbbell or barbell row. Chest press or push up. Lat pulldown or assisted pull up. | Seated row. Dumbbell shoulder press. Tricep and bicep accessory. | 3 to 4 sets of 8 to 12 reps |
| Session C | Full body or posterior chain focus | Conventional deadlift. Single-leg Romanian deadlift. Dumbbell press. | Plank and core work. Step-ups or split squat. Face pulls or rear delt work. | 3 to 4 sets of 8 to 12 reps |
Rest 60 to 90 seconds between sets on primary movements. Progress the load when you can complete all sets and reps with good form and two to three repetitions still available. Do not chase soreness as a marker of a good session. Chase progressive overload over time.

Nutrition to Support Resistance Training for Women
The most common nutritional error among women who begin resistance training is failing to eat enough to support the adaptation they are trying to create. The fear of eating more, particularly of eating more protein and carbohydrate, undermines the results of the training and leaves women wondering why the programme is not working when in fact it is the fuel strategy that is failing.
Protein is the most critical macronutrient for women who lift. A target of 1.6 to 2 grams per kilogram of bodyweight per day provides the amino acids required for muscle protein synthesis in the hours following training. This applies equally to plant-based women: soy protein isolate and pea protein have been shown to be equivalent to whey protein for muscle protein synthesis outcomes when total leucine content is matched (4). Tofu, tempeh, edamame, lentils, chickpeas, and soy milk are the dietary building blocks of a plant-based protein strategy for lifting women.
Carbohydrates are the primary fuel source for resistance training and restricting them excessively undermines training performance, recovery, and hormonal function. Women who train with weights require sufficient carbohydrate to support the glycolytic energy demands of resistance exercise and to replenish muscle glycogen in the recovery window. Oats, sweet potato, brown rice, quinoa, lentils, and fruit are the practical carbohydrate sources that fuel training without the blood glucose volatility of refined alternatives.
Post-workout nutrition within two hours of a session is the practical window during which muscle protein synthesis is most responsive. A meal or snack containing twenty-five to forty grams of protein alongside complex carbohydrate is the evidence-supported target. For plant-based women, a soy protein or pea protein shake with oats, a tofu bowl with rice, or a lentil and sweet potato meal all meet this requirement effectively.
Top Tip
If you are training with weights three to four times per week and your performance, energy, and recovery are suffering despite consistent training, look at your protein and total calorie intake before looking at your programme. Underfuelling is the most common reason women do not make progress from well-designed resistance training. The food is not working against you. It is the material from which your results are built.
The Bone Density Case for Resistance Training: A Non-Negotiable Across Every Decade
I want to devote specific attention to bone density because it is perhaps the most important and least emotionally resonant argument for women starting resistance training. The results you see in the mirror matter. But the bone density you are building or failing to build right now will determine whether you fracture a hip in your 70s. That matters considerably more.
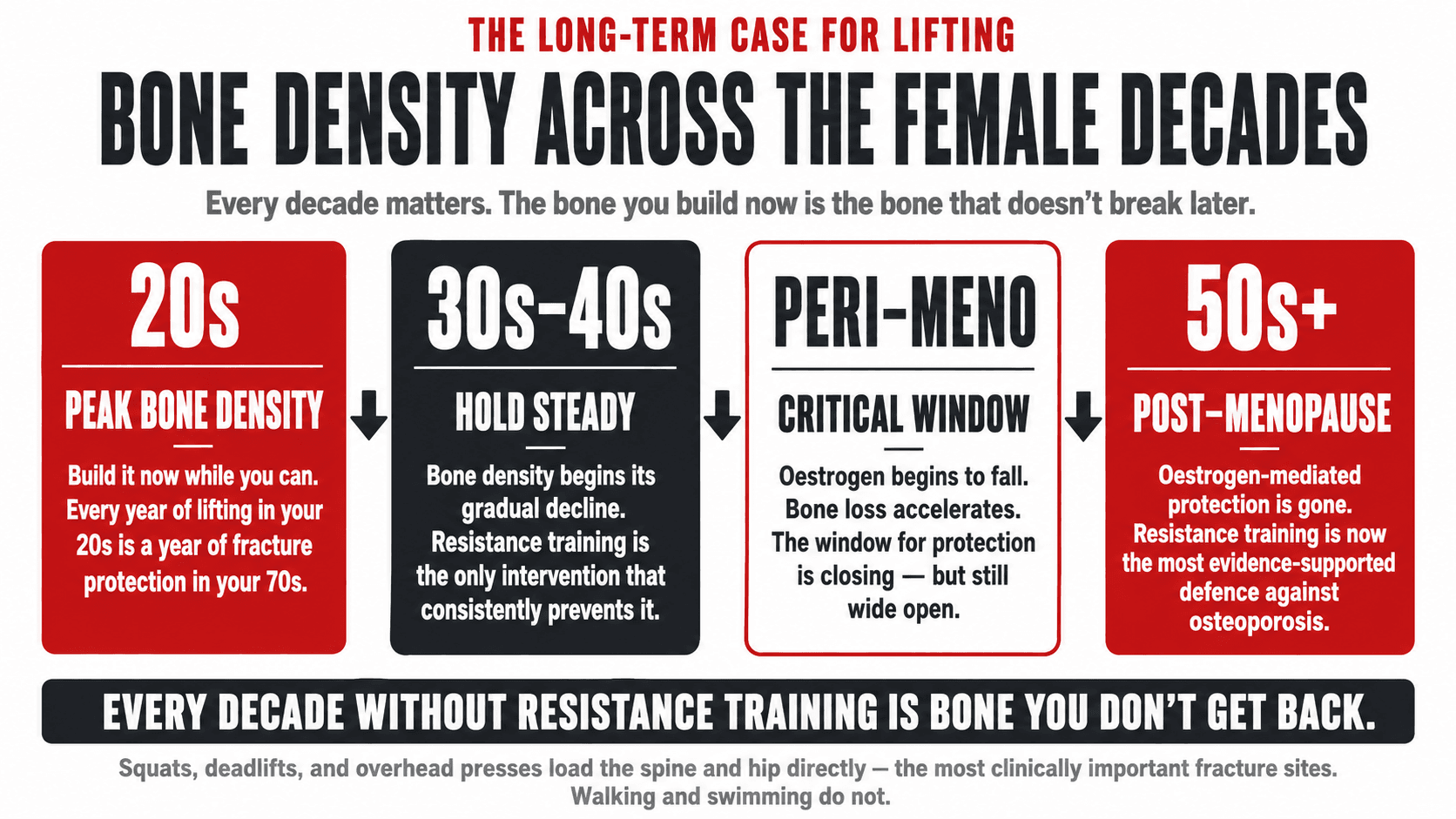
Bone density peaks in women in their late 20s and declines gradually thereafter, with an accelerated rate of loss in the years around menopause due to oestrogen withdrawal. Resistance training stimulates bone formation through mechanical loading: the force transmitted through bone during weighted exercises signals osteoblasts, the cells responsible for bone formation, to increase bone mineral density. This effect is site-specific, meaning that exercises that load the spine and hip, the most clinically important fracture sites, produce the most relevant bone density improvements (5).
Research has demonstrated that resistance training programmes of six to twelve months produce statistically significant improvements in bone mineral density at the spine and hip in premenopausal and postmenopausal women alike. This finding is particularly important for postmenopausal women, for whom oestrogen-mediated bone protection has been withdrawn and for whom the rate of bone loss without intervention is clinically significant.
Walking, swimming, and cycling, which many women rely on as their primary exercise, are insufficient stimuli for bone density maintenance at the hip and spine because they do not generate the mechanical loading required to activate the bone remodelling response in these sites. Resistance training does. This is one of the reasons that replacing or supplementing low-impact cardio with resistance training is a public health intervention, not just a body composition preference.
Top Tip
Squats, deadlifts, and overhead presses load the spine and hip directly and produce the most relevant bone density stimulus for fracture prevention. If you have a family history of osteoporosis, have been told you have low bone density at any point, or are approaching or past menopause, resistance training is not optional for your long-term health. Have a conversation with your GP about a DEXA scan if you have not had one and are over 50, or earlier if you have risk factors.
What Women Who Start Lifting Actually Experience
I am going to speak from my experience coaching women across more than fifteen years rather than from a research paper here, because I think it is worth naming what the subjective experience of resistance training actually looks like for women who commit to it.
The first thing most women notice is not the physical change. It is the change in how they feel about their body. The shift from measuring progress by how little space they take up to measuring it by what their body can do is one of the most profound psychological changes I witness in coaching. A woman who can deadlift her own bodyweight relates to her body completely differently than the same woman whose relationship with it has been defined by calorie restriction and the number on the scale.
The physical changes follow consistently: a leaner waistline, improved shoulder and back definition, stronger legs, better posture. These changes happen without the scale necessarily moving significantly, which initially surprises most women and then, once they understand why, becomes one of the most motivating discoveries of the process. The body is changing in every direction that matters. The scale is just not the instrument that can see it.
Every woman I have coached who committed to resistance training with genuine effort and consistency has said some version of the same thing at some point. They wish they had started sooner. Not because the years before were wasted, but because the experience of feeling strong, capable, and genuinely well in their body is one they want more of.
Top Tip
Take measurements and photographs at the start of your resistance training programme, not just scale weight. Measure your waist, hips, and upper arms. Note how your clothes fit. These markers will show you the changes that the scale cannot, and they will sustain your motivation through the early weeks when the scale may not move in the direction you expect. The composition change is real and meaningful. You need the right measurement tools to see it.
How I Introduce Women to Resistance Training
Every new female client I work with begins with a movement assessment and a programme built around the compound foundation I have described in this article. Regardless of whether a woman has never touched a barbell or has years of training behind her, the starting point is always the same: establish the fundamental movement patterns, build confidence under load, and create the progressive overload framework that produces results that compound over months and years.
For women who are new to lifting, the first six to eight weeks are about technique, familiarity, and building the neuromuscular patterns that make heavier loading safe and effective. Results begin during this period but accelerate significantly once the movement patterns are established and load can be added progressively. The compounding effect of resistance training over years is among the most powerful health investments available to a woman, and I have the privilege of witnessing it consistently across every client category I work with.
If you are ready to start, or to do it properly for the first time, I work one-to-one with women online globally. The programme will be built around your specific goals, your starting point, your dietary background, and your life. No treadmills as a substitute for the training your body actually needs.
