The Question Nobody Asks Themselves Honestly
The two-path projection for health is the most direct and most emotionally confronting tool I use in any coaching conversation. It is not complicated. It does not require a framework or a model. It requires only the willingness to ask two questions with complete honesty and to sit with the answers long enough for them to generate the decision they almost always point toward.
The first question is: if I continue doing exactly what I am currently doing, in precisely the way I am currently doing it, where will I realistically be in five years? Not where I hope to be. Not where I might be if some circumstances change or some motivation arrives. Where will I be if nothing changes, the current trajectory continues uninterrupted, and five years pass? In terms of my body, my energy, my health markers, my physical capability, my relationship with food, my weight, my risk of the chronic diseases that are accumulating slowly in the background of the life I am currently living.
The second question is: if I make a specific, meaningful change now and apply it consistently across those same five years, where could I realistically be instead? Not a fantasy. A realistic, evidence-based projection of what consistent application of the right approach produces over five years in a person with my starting point.
These two questions, placed side by side, produce a comparison that is almost always the most motivationally powerful moment in any initial coaching conversation. Not because the answer to the second question is inspiring, though it is. Because the answer to the first question is uncomfortable in a way that motivational content about the second path alone never produces. The gap between the two trajectories, made explicit and personalised, is the most honest and accurate picture of what is actually at stake in the health decisions being made today.
Why the Present Moment Always Feels Neutral When It Is Never Neutral
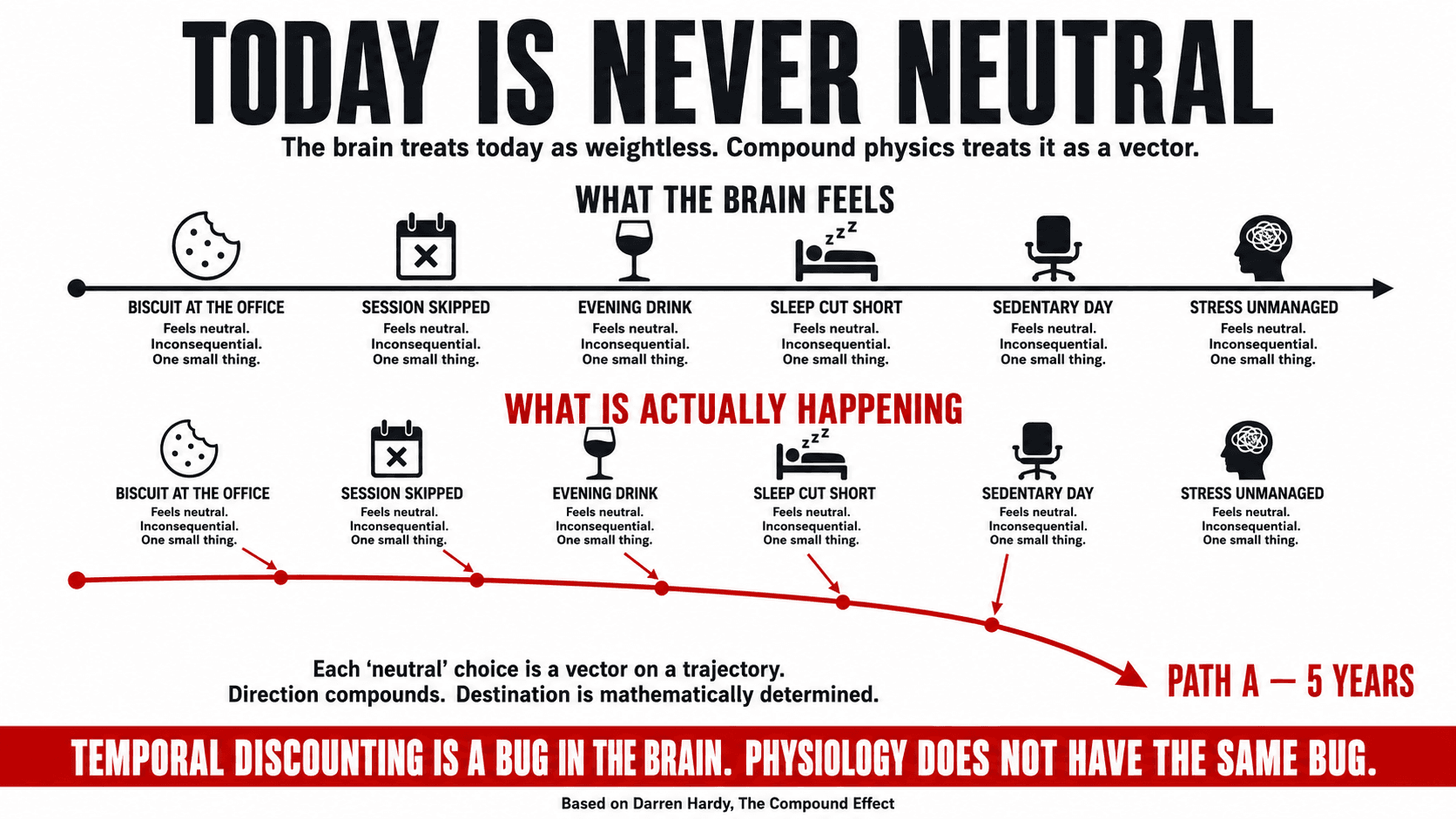
The brain is systematically biased toward the present. This is not a character flaw. It is a feature of temporal discounting, the neurological tendency to weight immediate costs and benefits more heavily than delayed ones. A treat that is available now is experienced as more valuable than a health outcome that is available in five years. A training session that requires effort now is experienced as more costly than the energy and metabolic health available in five years if it is attended consistently. The present moment has enormous representational weight in the brain's decision-making architecture, and the future has very little.(1)
The consequence is that most people make health decisions as though today is neutral: as though the biscuit taken from the office kitchen, the session skipped because of tiredness, the evening alcohol that has become an unremarkable daily ritual, the sleep cut short for the television, the sedentary workday unbroken by any movement, are each small, inconsequential, neutral acts. They are not neutral. Each one is a decision point on a trajectory that is going somewhere specific. And the trajectory's destination, while invisible in the present moment, is as mathematically determined by today's decisions as a ship's position after two weeks of sailing is determined by the bearing set at departure.
Darren Hardy's compound effect framework makes the same argument with precision: the choices that determine a person's long-term health are almost never the dramatic ones. They are the small, daily, unremarkable ones that individually appear inconsequential and collectively constitute the trajectory. The person who eats slightly better, moves slightly more, sleeps slightly longer, and manages stress slightly more intelligently every day for five years does not have a slightly better health outcome than the person who does not. They have a categorically different health profile, a different body composition, a different metabolic age, and a measurably different risk relationship with the chronic diseases whose probability is being set by daily decisions the person believes are neutral.(2)
“The difference between successful people and really successful people is that really successful people say no to almost everything.”
— Warren Buffett
Key Insight: Ask yourself, about a specific recurring health behaviour you have been tolerating rather than addressing: if I continue doing this at the current frequency, for the next five years, what is the realistic destination? Give the destination a specific description. The sedentary afternoon. The worsening metabolic markers. The accumulating visceral fat. The energy level at 52 that is lower than it was at 42. Specificity is uncomfortable. It is also what converts the question from an abstract exercise into a genuine decision.
The Two-Path Fork: What the Diverging Trajectories Actually Look Like Across Five Years
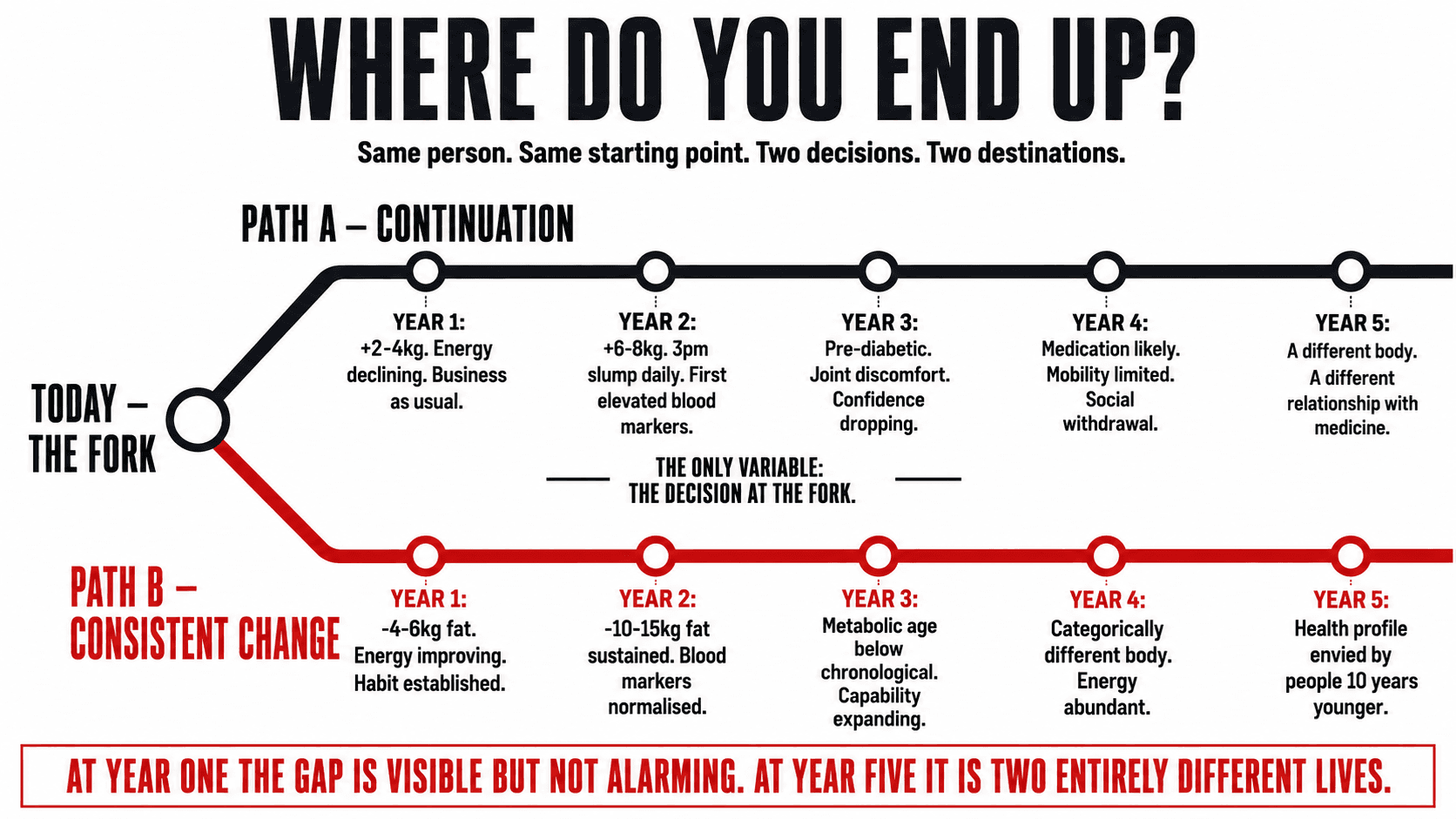
The diagram below maps the two-path projection across five years for a person at a common starting point: moderately overweight, sedentary, energy declining, blood markers drifting in the wrong direction, not yet experiencing clinical disease but heading toward it. One path continues the current trajectory. The other represents the application of a structured, consistent health programme. The gap between them at each year is not a motivational exaggeration. It is a realistic projection based on the established physiology of incremental neglect and incremental improvement.
Diagram
The Two-Path Fork — Same Person, Same Starting Point, Two Different Decisions
| Year | Path A — Continuation — Nothing Changes | Path B — Consistent Change — Applied Now |
|---|---|---|
| TODAY — THE FORK POINT — Both paths begin here, from the same person, the same body, the same history. The only variable is the decision made today and repeated. | ||
| Year 1 | Early signs continue. Low energy. Creeping weight gain of 2-4kg. No deterioration dramatic enough to demand attention. Business as usual. | First visible adaptations. Energy improving. 4-6kg of body fat lost. Training habit established. Sleep quality measurably better. Earliest blood marker improvements. |
| Year 2 | Weight now 6-8kg above starting point. Energy lower. 3pm slump daily. First elevated blood glucose readings. GP monitoring cholesterol. Motivation for change harder to access. | Body composition transformation consolidated. 10-15kg of fat lost and sustained. Resting heart rate improved. Blood markers normalised. Training is now a permanent habit rather than an effort. |
| Year 3 | Pre-diabetic blood glucose range. Hypertension emerging. Sleep disrupted by weight. Joint discomfort limiting mobility. Doctor's appointments more frequent. Confidence declining. | Metabolic age measurably lower than chronological age. Sustained lean body composition. Blood pressure in optimal range. High daily energy. Physical capability expanding not contracting. |
| Year 4 | Prescription medication for blood pressure or blood glucose likely. Significant mobility limitations. Energy insufficient for physical activity. Social withdrawal around body image. | A person who looks, moves, and feels genuinely different from the year-zero starting point. Not just lighter. Categorically more capable, energetic, and metabolically healthy. |
| Year 5 | A different body, a different health profile, and a different relationship with medicine, movement, and daily energy than the person who took Path B five years earlier. The same starting point. An entirely different destination. | Five years of compound physical improvement. A health profile that is the envy of people a decade younger. An identity anchored in health rather than struggling against its absence. The investment made in year one compounding visibly. |
| Same starting point. Same five years. The only variable is the decision at the fork. At year one the gap is visible but not alarming. At year five it is the difference between two entirely different lives, two entirely different bodies, and two entirely different relationships with physical capability and health. | ||
The Physiology of Incremental Neglect: What the Continuation Path Is Building Right Now
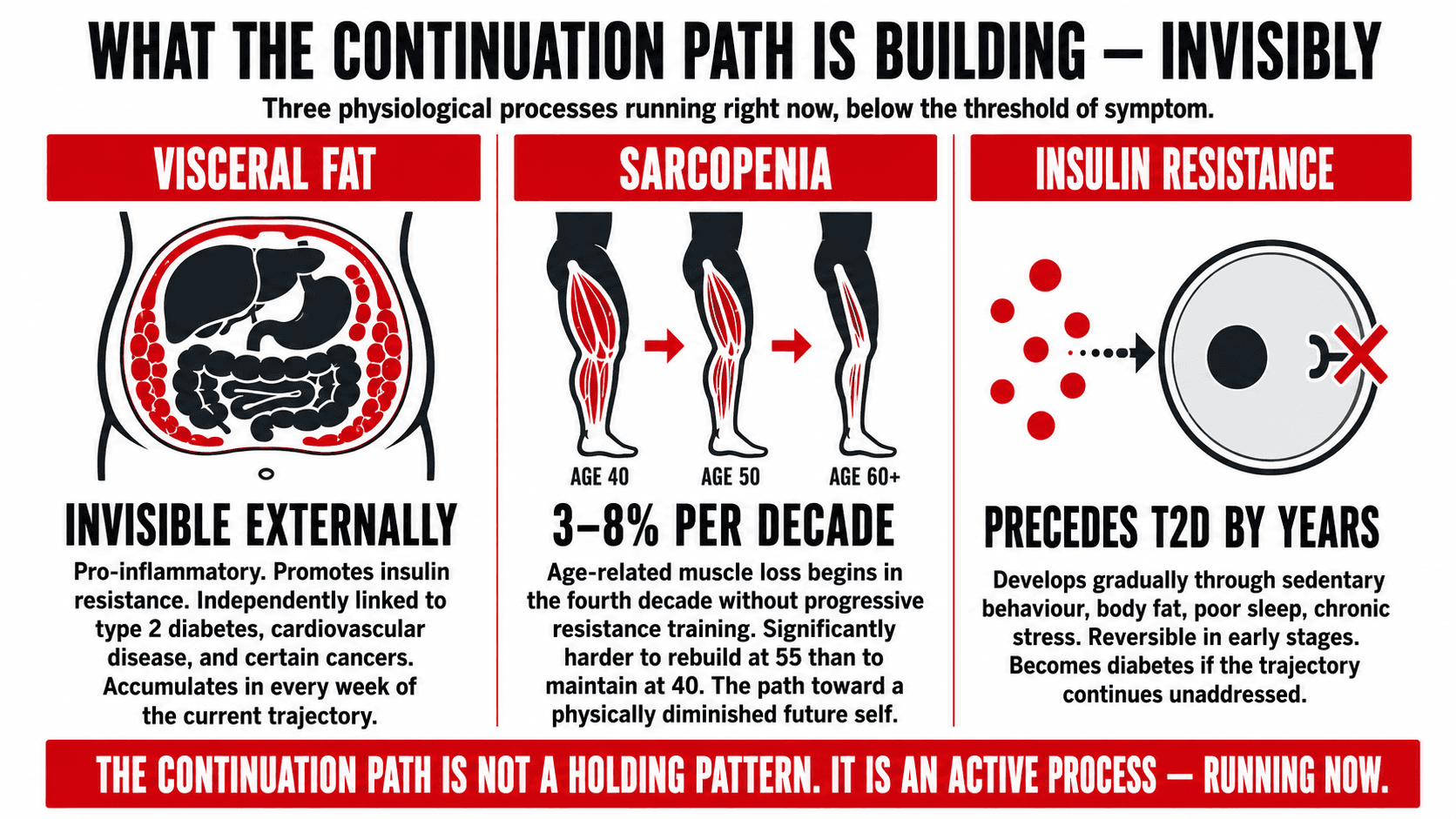
The continuation path is not a static holding pattern. It is an active process of physiological change in a specific and well-documented direction. Understanding what is accumulating on Path A, below the threshold of immediate symptom, makes the two-path projection more precise and more motivationally significant than the abstract concept of getting worse over time.
Visceral adipose tissue — the fat that accumulates around the internal organs in the abdominal cavity rather than subcutaneously — is the most metabolically active and most clinically significant form of excess body fat. It is also largely invisible: a person can have a dangerously elevated visceral fat level with only moderate visible changes to their external appearance. Visceral fat is pro-inflammatory, metabolically active in ways that promote insulin resistance, and independently associated with elevated risk of type 2 diabetes, cardiovascular disease, and certain cancers. It accumulates slowly, invisibly, and compounds. The continuation path is building it, a small amount at a time, in every week that the current trajectory continues.(3)
Sarcopenia — the age-related loss of muscle mass — begins in the fourth decade of life in adults who do not train with progressive resistance exercise. The rate of loss is approximately 3-8% of muscle mass per decade without intervention, accelerating after the age of 60 to rates that meaningfully affect mobility, metabolic rate, and functional independence. The person on the continuation path who is not engaged in progressive resistance training is losing muscle that will be significantly harder to rebuild at 55 than it would be to maintain at 40. The continuation path is not simply a trajectory toward poor health outcomes. It is a trajectory toward a physically diminished version of the future self.(4)
Insulin resistance develops gradually through the combination of sedentary behaviour, excess body fat, poor sleep, and chronic low-grade stress. It precedes type 2 diabetes by years and in many cases decades, and is entirely reversible in its early stages through the same interventions that address the other elements of the continuation path: structured exercise, nutritional quality, weight management, and sleep. The person in the pre-diabetic range whose GP is monitoring their blood glucose is not at the beginning of a disease process. They are in its middle stages. The continuation path is the path toward medication. The change path is still the path toward reversal.(5)
Key Insight: Run the continuation path projection for your own specific health markers. Not in abstract terms. Take your most recent blood work, your current weight trajectory, your training frequency, your sleep duration, and your stress level. For each one, ask: if this continues in the direction it is currently moving for five years, what is the realistic destination? The projection does not require medical training. It requires honesty about the direction each variable is moving and the knowledge that directions compound.
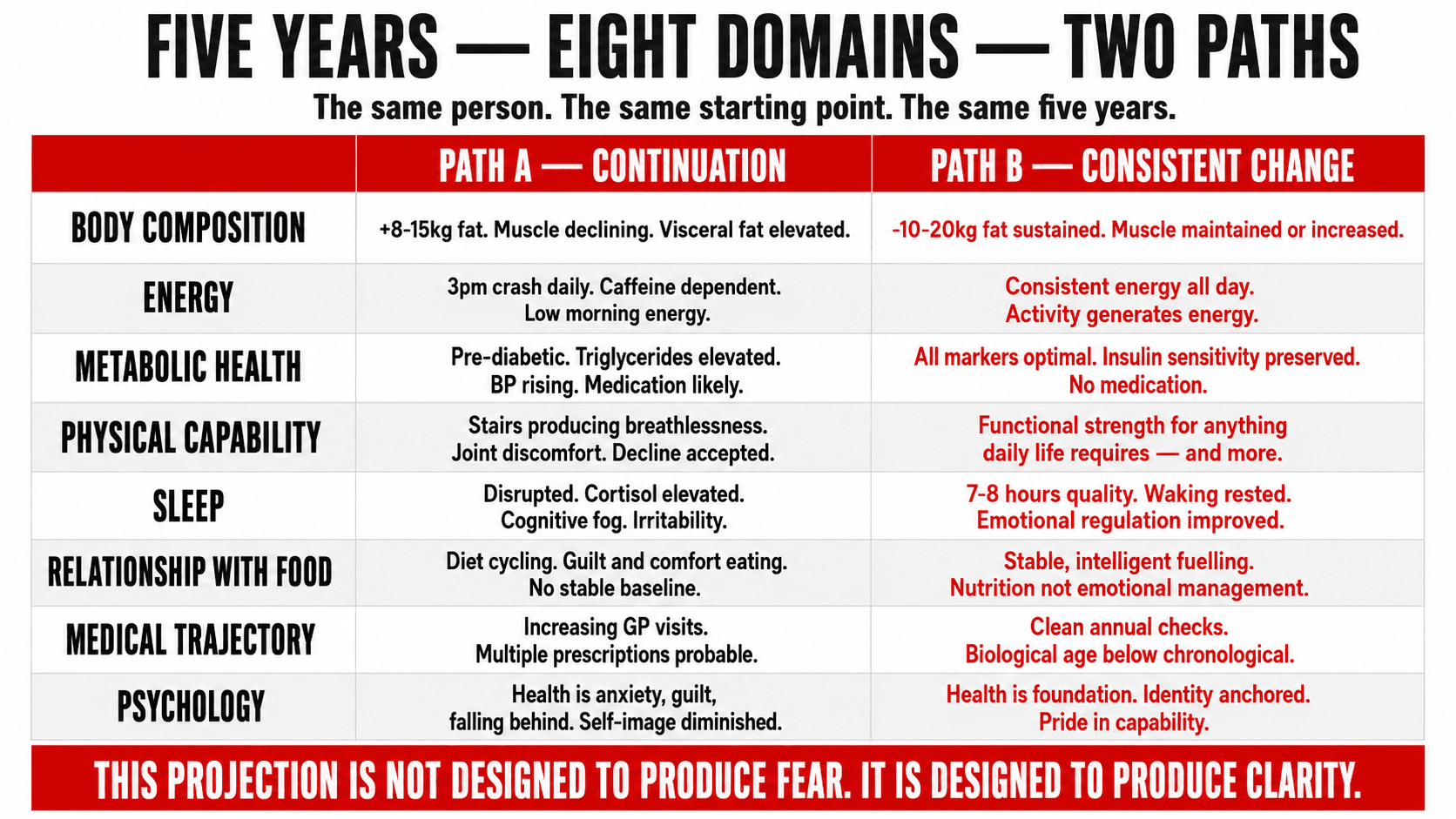
The Domain Projection: What Each Path Produces Across Eight Areas of Health
The two-path projection is most powerful when it is made specific across the individual domains of health that are most relevant to the person undertaking it. The table below maps both paths across eight health domains, from body composition to psychological relationship with health, for a person in their forties at a common starting point.
Table
The Two-Path Domain Projection — Where Each Path Leads Across Eight Health Areas Over Five Years
| Health Domain | Path A — Five Years of Continuation | Path B — Five Years of Consistent Change |
|---|---|---|
| Body composition | 8-15kg additional fat gain. Sarcopenic muscle loss beginning to affect metabolic rate and daily function. Visceral fat elevated. Clothes a persistent source of discomfort. | 10-20kg of fat lost and sustained. Muscle mass maintained or increased through progressive resistance training. Lean body composition that operates as a foundation, not a problem. |
| Energy and vitality | 3pm crash daily. Rising dependence on caffeine to function. Low morning energy. Increasing reliance on alcohol to decompress. Energy insufficient for physical activity outside work. | Consistent energy across the full day. No significant afternoon dip. Morning energy reliable. Physical activity generates rather than depletes energy. No dependence on stimulants to function. |
| Metabolic health | Fasting glucose likely in pre-diabetic range. Triglycerides elevated. HDL cholesterol declining. Blood pressure above optimal. GP monitoring and medication increasingly likely. | All metabolic markers in optimal clinical range. Insulin sensitivity maintained or improved. Blood pressure normalised through exercise and weight management. No medication required. |
| Physical capability | Climbing stairs producing breathlessness. Inability to perform activities requiring sustained physical effort. Joint discomfort limiting movement. Physical decline accepted as inevitable. | Functional strength for any activity daily life requires and more. Cardiovascular capacity that makes physical challenges manageable. Physical capability expanding rather than contracting. |
| Sleep quality | Sleep disrupted by weight-related issues, elevated cortisol, and alcohol dependency as sleep aid. Waking unrefreshed. Cognitive fog accumulating. Irritability affecting relationships. | Seven to eight hours of high-quality sleep. Waking rested. Cognitive function supported by adequate deep sleep and REM. Emotional regulation improved by sleep quality. |
| Relationship with food | Ongoing cycle of dietary discipline and compensation. Food a source of comfort, guilt, and recurring emotional conflict. No stable nutritional baseline. Relationship with food unchanged. | A stable, intelligent relationship with food based on understanding of what the body needs. Nutrition as fuel rather than emotional management. No diet cycling. No guilt. |
| Medical trajectory | Increasing number of GP appointments for conditions whose risk is directly modifiable by lifestyle. Potentially multiple prescriptions. Chronic disease risk profile elevated. | Annual health check producing clean results. Biological age measurably lower than chronological. GP relationship one of monitoring health rather than managing emerging disease. |
| Psychological relationship with health | Health as a persistent background source of anxiety, guilt, and a sense of falling behind. Each failed attempt adding to a narrative of inability. Self-image diminished. | Health as a foundation rather than a problem. Pride in the capability of the body. Identity anchored in being a healthy person rather than aspiring to become one. |
| This projection is not designed to produce fear. It is designed to produce clarity. Clarity about what is actually at stake in the daily decisions that feel neutral. Clarity about the compound destination of the trajectory currently in motion. | ||
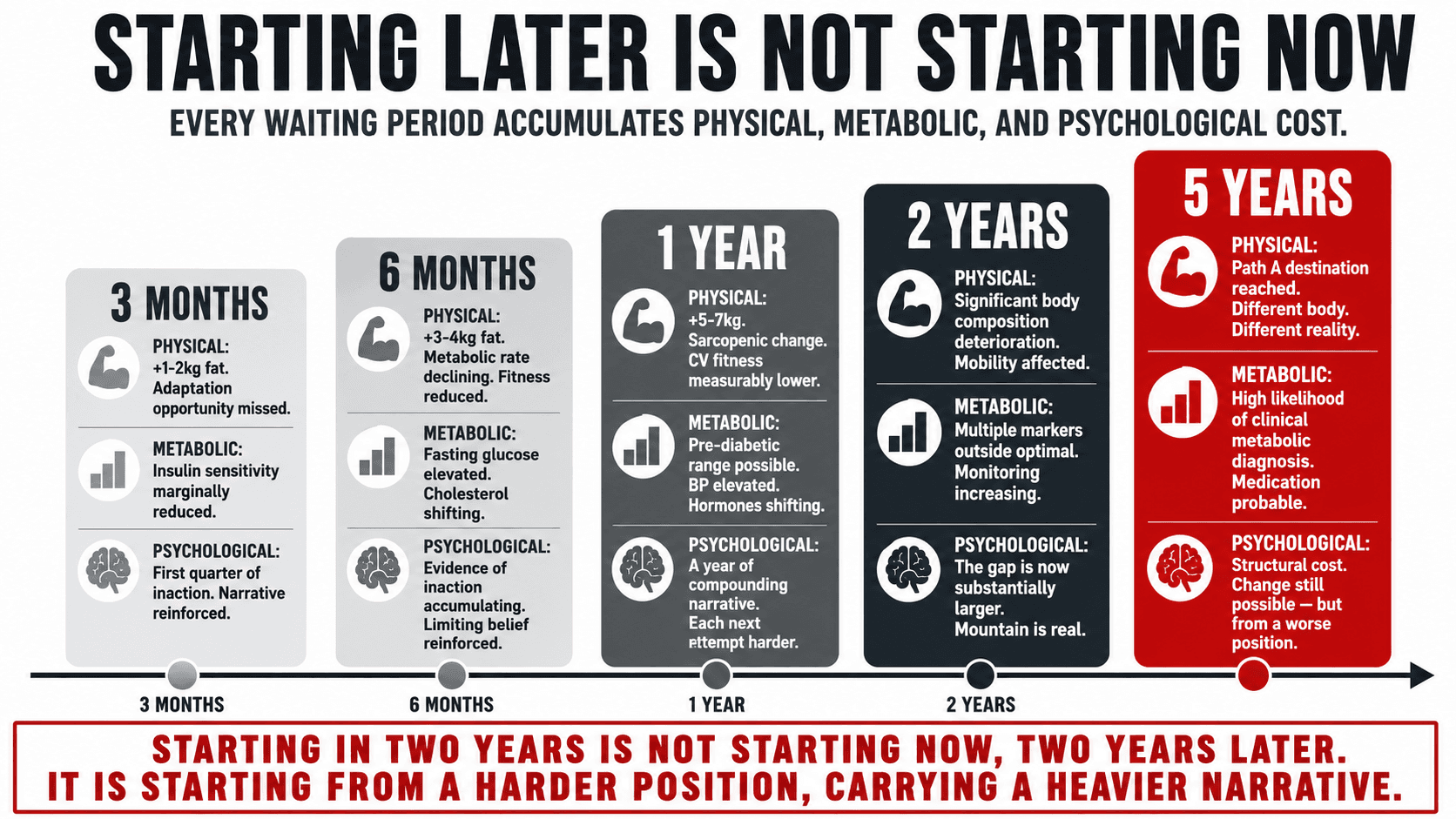
The Cost of Delay: Why Starting Later Is Not Equivalent to Starting Now
One of the most common cognitive distortions in health decision-making is the belief that starting later is equivalent to starting now, that the person who begins a health programme in two years will arrive at the same destination as the person who begins today, just two years behind. This belief is incorrect, and understanding precisely why it is incorrect is one of the most important arguments for making the change decision at the fork rather than deferring it.
Physical adaptation is time-dependent in ways that are not simply additive. The cardiovascular and metabolic adaptations produced by two years of consistent training compound on each other: the cardiac adaptations of year one create the baseline for the adaptations of year two, which would not have been available without year one. The muscle mass maintained through progressive resistance training in the forties protects against the accelerated sarcopenia of the fifties in ways that beginning training in the fifties, while still valuable, cannot fully replicate. The insulin sensitivity restored by weight management and exercise in the early stages of metabolic deterioration has a substantially better prognosis than the same intervention attempted after clinical diabetes has been established.
The psychological cost of delay is equally significant and less commonly acknowledged. Every month on the continuation path deposits additional evidence in the limiting belief file, makes the gap between current reality and desired health larger and more daunting, and compounds the narrative of inability that makes the next attempt harder before it begins. The person who starts the change path today is starting from a position where the gap is smaller, the narrative is less entrenched, and the compound return on the investment has the maximum available time to accumulate.
Table
The Cost of Delay — What Is Accumulated on Path A During Each Waiting Period
| Waiting Period | Physical Accumulation on Path A | Metabolic Accumulation on Path A | Psychological Cost of Continuing |
|---|---|---|---|
| 3 months | 1-2kg additional fat gain. No muscle loss yet measurable but progressive resistance adaptation opportunity missed. | Insulin sensitivity marginally reduced. Blood markers unchanged but trajectory direction set. | One quarter in which the gap between current state and desired state grew. Narrative of inaction reinforcing. |
| 6 months | 3-4kg additional fat gain. Metabolic rate beginning to decline with muscle mass changes. Physical fitness measurably reduced. | Fasting glucose marginally elevated in susceptible individuals. Cholesterol profile shifting. | Six months of evidence that change did not happen despite intention. Limiting belief reinforced. Next attempt harder. |
| 1 year | 5-7kg additional fat gain likely. Sarcopenic change beginning in fourth decade adults. Cardiovascular fitness measurably lower. | Pre-diabetic range increasingly possible in susceptible individuals. BP elevated. Hormonal profile shifting. | A year of compounding narrative. The person who wanted to change and did not. Each subsequent attempt carries the weight of the previous ones. |
| 2 years | Significant body composition deterioration. Mobility beginning to be affected. Physical activity more difficult and less enjoyable. | Multiple metabolic markers likely outside optimal range. Medical monitoring increasing. | The gap is now substantially larger than at the fork point. The mountain is real. The narrative of inability is deeply reinforced. |
| 5 years | The destination described in Path A of the fork diagram above. A different body and a different physiological reality from the one that existed at the fork. | High likelihood of clinical metabolic diagnosis. Medication probable. Disease risk profile substantially elevated. | The cost of not deciding at the fork, compounded across five years, is now structural. The change is still possible. But it is harder, slower, and begins from a worse position. |
| The cost of delay is not simply the delay. It is the physical, metabolic, and psychological accumulation that occurs during the delay. Starting in two years is not starting now, two years later. It is starting from a harder position, with a larger gap, carrying a heavier narrative. | |||
The Change Decision Is Made Exactly Once: What Choosing Path B Actually Requires
The most important thing to understand about the change decision is its structure. It is not a series of daily decisions to be remade every morning against the resistance of inertia and the availability of the easier option. It is a single decision made once at the fork that then generates a series of daily actions whose execution is supported by the habit architecture, the identity work, the environment design, and the goal structure described throughout this series.
Viktor Frankl's observation that between stimulus and response there is a space, and in that space lies the human capacity to choose, applies precisely to the fork point. The stimulus is the current situation: the health trajectory in motion, the accumulating physiological changes, the compound destination becoming clearer. The response is the continuation path, the default, requiring no decision because it is simply what happens when nothing changes. In the space between them is the fork. The change decision is made in that space, once, with a clarity that does not require repeated renewal if the architecture that supports it is properly built.(6)
What choosing Path B requires is not a dramatic life overhaul or a commitment to perfection. It requires a starting programme that is achievable and evidence-based, an environment designed to support the programme rather than undermine it, a habit architecture that removes the daily decision from the healthy behaviour, a goal structure built on purpose and identity rather than outcome anxiety, and the belief that the destination described in the right column of every table in this article is genuinely available. Not to someone else with better genetics, more time, or more natural discipline. To this person. At this starting point. With this history. Now.
“In any moment of decision, the best thing you can do is the right thing. The worst thing you can do is nothing.”
— Theodore Roosevelt
Key Insight: The two-path projection exercise works most powerfully when it is written rather than thought. Take a piece of paper, draw a vertical line down the middle, write Path A on the left and Path B on the right, and spend twenty minutes filling in both sides with specific, honest projections across the health domains most relevant to your own situation. What you write in the left column is the argument for making the change. What you write in the right column is the destination you are navigating toward. Keep the paper. Read both columns when motivation is absent, because the question it answers is more durable than any motivational state.
The Conversation That Starts Every Programme
The two-path projection is a conversation I have at the beginning of every new coaching relationship, because it establishes the stakes more honestly and more precisely than any goal-setting exercise alone. Setting a goal points toward a desired destination. The two-path projection shows both destinations simultaneously and makes the cost of remaining on the continuation path explicit and personal.
I have sat with clients who arrived having tried repeatedly, who had accumulated a significant narrative of failure, and who were not fully convinced that the change path was genuinely available to them. The two-path projection, run honestly across their specific health markers, their current trajectory, and the five-year destination of both paths, produced a clarity and a motivation that no goal-setting exercise had previously generated. Not because the right column was inspiring, though it was. Because the left column was honest in a way that could not be argued with.
The fork exists right now. Not in the future when circumstances are more convenient. Not after the holiday, the busy period, the January reset. Now. The person reading this article is at the fork. The question is not whether to choose. The choice is already being made by default if no explicit decision is made. The question is which path to take. I work one-to-one with clients online globally. The two-path conversation is where the programme begins.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- Thaler RH. Misbehaving: The Making of Behavioural Economics. London: Penguin; 2015.
- Hardy D. The Compound Effect: Jumpstart Your Income, Your Life, Your Success. New York: Vanguard Press; 2010.
- Grundy SM. Metabolic syndrome pandemic. Arteriosclerosis, Thrombosis, and Vascular Biology. 2008; 28(4): 629-636.
- Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age and Ageing. 2019; 48(1): 16-31.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. New England Journal of Medicine. 2002; 346(6): 393-403.
- Frankl VE. Man's Search for Meaning. Boston: Beacon Press; 1959.
- Hershfield HE. Future self-continuity: how conceptions of the future self transform intertemporal choice. Annals of the New York Academy of Sciences. 2011; 1235(1): 30-43.