
The Deficiency That Drains a Woman's Energy Before She Even Knows It Has Started
Iron deficiency in women is the most common nutritional deficiency in the world, and women bear a disproportionate share of its burden. Premenopausal women lose iron through menstruation every month. Women who eat plant-based diets have lower access to haem iron, the most efficiently absorbed form. Women who exercise at moderate to high intensity have elevated iron requirements from increased red blood cell turnover and gastrointestinal losses. Women who are pregnant or breastfeeding have substantially elevated requirements that are frequently unmet. The list of factors that place women at risk for iron deficiency is long. The medical attention given to iron status in otherwise healthy women is consistently insufficient.
The insidious quality of iron deficiency is that its symptoms are accepted. Fatigue, poor concentration, reduced motivation, breathlessness on exertion, feeling cold, and a training performance that never quite reaches what it should: these are the symptoms that most women attribute to stress, poor sleep, doing too much, or simply being tired in the way that modern life makes people tired. They are not always those things. They are frequently the measurable consequence of ferritin levels that are technically within the normal range but nowhere near the levels at which the body functions optimally.
This article explains the difference between iron deficiency and iron deficiency anaemia, why ferritin is the marker that matters and why most women are never told to check it, what the symptoms of suboptimal iron status actually are, and what the dietary and supplemental approach looks like for women of every dietary background.
Iron Deficiency vs Iron Deficiency Anaemia: The Distinction That Changes Everything
The most important concept in understanding iron status in women is the difference between iron deficiency and iron deficiency anaemia, because most clinical assessment focuses on the latter while the former is responsible for most of the symptoms women experience.
Iron deficiency anaemia is the end stage of a progressive depletion process in which iron stores have fallen so low that haemoglobin production is impaired and red blood cells become smaller and less functional. It is diagnosed when both haemoglobin falls below normal and red blood cell indices are abnormal. It is the most obvious and most severe presentation of iron depletion, and it is the one that most GPs are looking for when they order a full blood count.
Iron deficiency without anaemia occurs earlier in the depletion process, when ferritin (the body's iron storage protein) has fallen to levels that impair iron-dependent functions throughout the body, but before haemoglobin is significantly affected. A woman with a ferritin of 12 micrograms per litre technically falls within some laboratory normal ranges but may be experiencing significant fatigue, poor cognitive function, reduced exercise tolerance, and impaired mood because the functional iron available for non-haematological processes is insufficient. This presentation is extremely common in premenopausal women and is frequently missed because the haemoglobin looks normal (1).
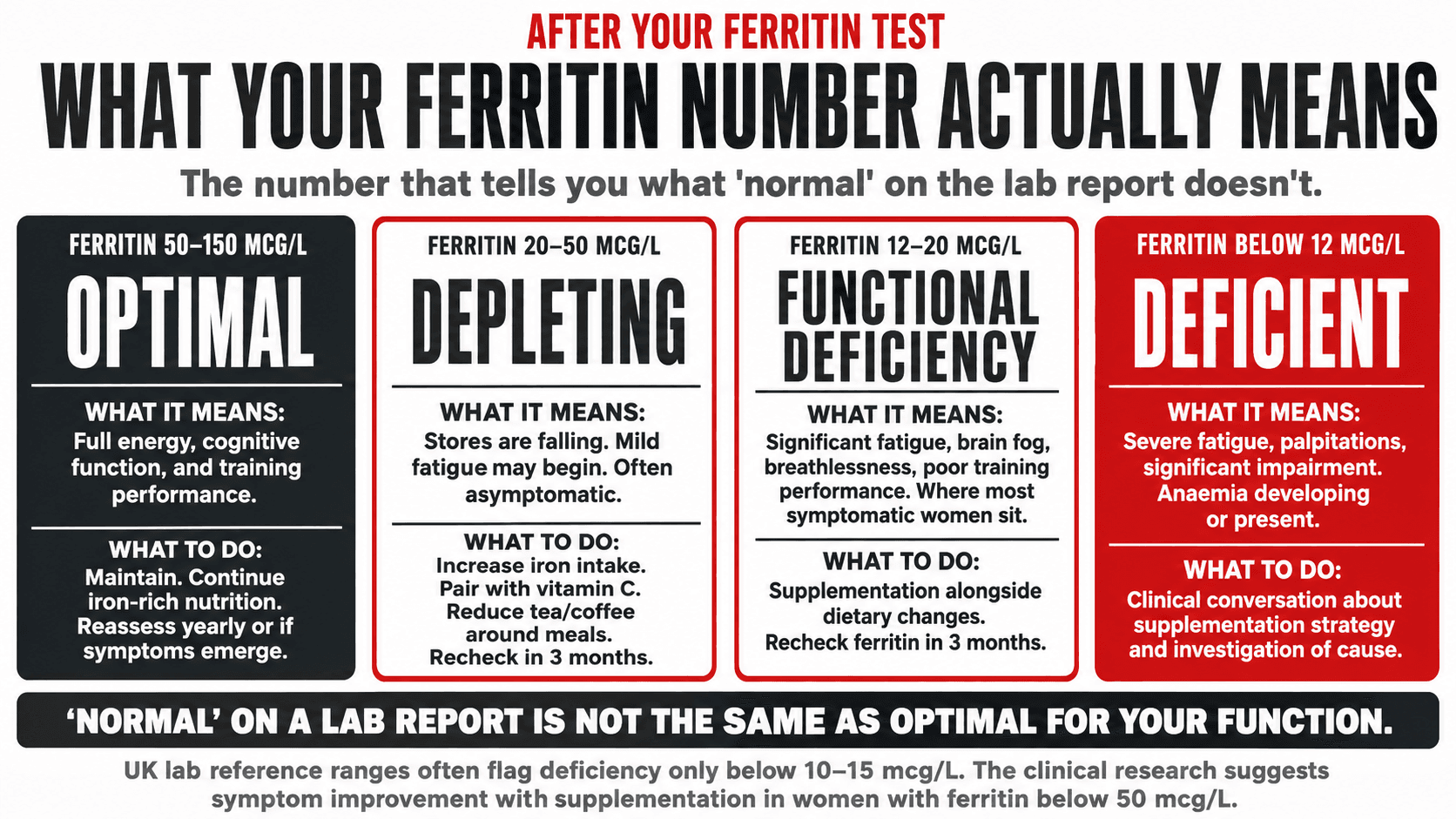
The clinical research consistently indicates that fatigue and cognitive symptoms associated with iron deficiency can be present and clinically meaningful at ferritin levels well above those that produce anaemia. Studies have demonstrated symptom improvement with iron supplementation in women with ferritin below 50 micrograms per litre who had normal haemoglobin, suggesting that the threshold for functional iron sufficiency is considerably higher than the threshold for diagnosing anaemia (2). This matters enormously for how women interpret their blood test results and how they advocate for appropriate assessment.
THE IRON DEPLETION CONTINUUM
From Optimal to Anaemia
01
Optimal Iron Status
Ferritin: 50–150 mcg/L
Haemoglobin normal. Full energy, cognitive function, and exercise performance. No iron-related symptoms.
02
Stage 1: Storage Depletion
Ferritin: 20–50 mcg/L
Ferritin falling. Haemoglobin still normal. Mild fatigue may begin. Often asymptomatic. Correctable through dietary intervention.
03
Stage 2: Functional Iron Deficiency
Ferritin: 10–20 mcg/L
Haemoglobin still technically normal. Significant fatigue, brain fog, breathlessness on exertion, poor training performance, mood low, cold intolerance. This is where most symptomatic women sit and where most GPs say ‘your blood tests are normal’.
04
Stage 3: Iron Deficiency Without Anaemia
Ferritin: below 12–15 mcg/L
Haemoglobin still within range but erythropoiesis is affected. Severe fatigue, palpitations, difficulty with any exertion, significantly impaired cognitive function. Requires supplementation, not dietary change alone.
05
Iron Deficiency Anaemia
Ferritin: very low
Haemoglobin below 120 g/L in women. Red cells small and pale (microcytic hypochromic). Debilitating symptoms. Requires supervised supplementation and investigation of cause. This is what most GPs are looking for. Most women with iron-related fatigue never reach this stage — they suffer at Stage 2 and 3, where they are told they are fine.
If your GP says your iron levels are normal but you have the symptoms described at Stages 2 and 3, ask specifically for your ferritin number. A result within the laboratory reference range is not the same as optimal for energy, performance, and wellbeing.
Top Tip: When your GP orders an iron blood test, ask for ferritin specifically alongside the standard full blood count. Many routine blood panels do not include ferritin unless it is requested separately. A ferritin result gives you the most clinically useful picture of your iron storage status. If your ferritin is below 30 mcg/L and you have fatigue, ask for a repeat test and a clinical conversation about whether supplementation is appropriate. ‘Normal’ on a lab report means within the reference range, not optimal for your function.
Symptoms of Iron Deficiency: What to Look For
The symptom profile of iron deficiency at functional levels, before frank anaemia develops, is one of the most commonly misattributed in women's health. Because the symptoms overlap with stress, poor sleep, overwork, and depression, they are frequently addressed at the wrong level, with lifestyle changes and mental health support, when the underlying driver is nutritional.
| Symptom Domain | Stage 1 — Storage Depletion | Stage 2 to 3 — Functional Deficiency | Stage 4 — Anaemia |
|---|---|---|---|
| Energy and fatigue | Mild fatigue that is easy to attribute to other causes. May not be noticeable. | Persistent fatigue disproportionate to activity level. Waking tired despite adequate sleep. Energy crashes. | Debilitating fatigue. Difficulty with basic daily activities. Fatigue on minimal exertion. |
| Cognitive function | Subtle. May notice slightly slower thinking or mild difficulty concentrating. | Brain fog, difficulty concentrating, poor memory, reduced word retrieval speed, lower motivation. | Significant cognitive impairment. Difficulty with complex tasks. Mood substantially affected. |
| Exercise performance | Minimal impact. Slight reduction in peak performance may not be measurable subjectively. | Noticeably reduced aerobic capacity. Faster breathing at moderate effort. Training feels harder than it should. Slower recovery between sessions. | Breathlessness on light exertion. Palpitations during exercise. Exercise substantially impaired. |
| Physical signs | Often absent. Mild pallor occasionally. | Cold hands and feet. Pale inner eyelids and nail beds. Brittle nails. Hair shedding increase. Headaches. | Clearly pale skin and mucous membranes. Brittle nails, spoon-shaped nails (koilonychia). Significant hair loss. Restless leg symptoms. |
| Mood and sleep | Minimal impact. | Low mood, irritability, reduced motivation. Restless legs interfering with sleep. | Depression-like symptoms. Significantly disrupted sleep from restless leg syndrome. |
The most important clinical point: the majority of women with iron-related symptoms are at Stage 2 to 3, where haemoglobin is normal and a full blood count returns unremarkable. Ferritin is the marker that identifies this stage. Request it by name.
Why Women Are at Disproportionate Risk and Who Is at Greatest Risk
Iron deficiency is not randomly distributed across the female population. Specific groups face substantially elevated risk, and understanding where you sit in that risk landscape determines how proactively you need to approach your iron status.
Premenopausal women lose between 30 and 80ml of blood per menstrual period, representing approximately 15 to 40mg of iron per cycle. Women with heavy menstrual bleeding, defined clinically as blood loss greater than 80ml per cycle, lose substantially more. Replacing this iron from diet requires a daily intake of around 14.8mg, which is the UK recommended intake for women aged 19 to 50 and is considerably higher than the 8.7mg recommended for men and postmenopausal women. The gap between requirement and typical intake is wide for a significant proportion of premenopausal women, particularly those eating restricted diets (3).
Women eating plant-based diets face an additional challenge in iron absorption. Dietary iron exists in two forms: haem iron, found exclusively in animal foods, which is absorbed at 15 to 35%, and non-haem iron, found in plant foods, which is absorbed at 2 to 20% depending on the presence of absorption enhancers and inhibitors in the meal. A plant-based diet can provide adequate iron when planned thoughtfully, but requires considerably higher total iron intake to achieve the same absorbed quantity, and requires specific attention to the factors that enhance and inhibit absorption (4).
Active women who train regularly have iron requirements that are approximately 30 to 70% higher than sedentary women due to several mechanisms: increased red blood cell production to support elevated oxygen delivery, iron loss through sweat, gastrointestinal blood losses during endurance exercise, and haemolysis from the mechanical impact of foot striking in running. Women who combine heavy menstrual bleeding with regular endurance training are at particularly high risk and should have ferritin monitored regularly (5).
Pregnant women require approximately 27mg of iron per day due to expanded blood volume, placental needs, and fetal iron storage requirements. Postpartum iron depletion is common and frequently unaddressed, leaving many women in the months after delivery with a ferritin level that explains their significant fatigue but that is not consistently checked in postpartum care.
Top Tip: If you have heavy periods, defined as flooding through a pad or tampon in under two hours, passing clots larger than 50p coin, or bleeding for more than seven days, this is both a hormonal signal worth investigating (low progesterone relative to oestrogen is a common driver) and a significant iron loss that requires active dietary management. Bring both issues to your GP in the same appointment. The hormonal and iron-related conversations are inseparable in this context.

Iron-Rich Foods for Every Dietary Background: A Practical Reference
Iron cannot be stored in sufficient quantities to last more than a few months without dietary replenishment. Adequate daily intake from food is the foundation of iron status, and supplementation fills the gap when dietary intake alone is insufficient. The following table gives a complete practical reference for iron sources across all dietary backgrounds.
| Food Source | Iron per Serving (approx) | Type | Absorption Notes |
|---|---|---|---|
| Lentils (cooked, 200g) | 6.6mg | Non-haem. Excellent plant-based staple. Red, green, or Puy lentils all good sources. Versatile across cuisines. | Pair with vitamin C source: squeeze of lemon, tomatoes, or peppers in the same meal. Avoid tea or coffee within one hour. |
| Chickpeas (cooked, 200g) | 4.8mg | Non-haem. Excellent for all plant-based diets. Use in curries, salads, soups, or roasted as a snack. | Same as lentils. Pairing with vitamin C doubles or triples the absorbed iron. |
| Tofu, firm (100g) | 2.7mg | Non-haem. Good plant-based iron source alongside protein. Firm tofu is higher in iron than silken. Choose calcium-set for dual bone benefit. | Absorption enhanced by vitamin C. Avoid soy and phytate-rich foods reducing iron from the same meal if iron deficient. |
| Pumpkin seeds (30g) | 2.5mg | Non-haem. Excellent portable snack. Also rich in zinc and magnesium. Add to porridge, salads, or eat directly. | Pair with vitamin C containing foods. Good absorption when consumed with a meal. |
| Spinach (cooked, 100g) | 3.6mg | Non-haem. High raw volume required for a meaningful dose. Cooking concentrates iron content. Also contains oxalates that reduce absorption. | Oxalates in spinach reduce absorption. Pair with vitamin C and avoid as primary iron source when severely deficient. Variety of sources is better than spinach alone. |
| Dark chocolate (30g, 70% cocoa or above) | 3.4mg | Non-haem. Practical and enjoyable addition to iron strategy. Also provides magnesium. | Avoid eating with tea or coffee. Pair with vitamin C containing fruit. |
| Fortified breakfast cereal (40g) | Up to 8mg depending on brand | Non-haem (fortified). Highly variable between brands. Check the label. A useful contribution to overall intake, not a replacement for whole food sources. | Pair with orange juice at the same meal. Avoid tea or coffee within one hour. |
| Beef, lean (100g, cooked) | 2.7mg | Haem. Omnivore option. Haem iron is absorbed at 15 to 35% regardless of enhancers or inhibitors. Red meat two to three times per week is a practical iron strategy for omnivore women. | Haem iron absorption is largely independent of meal composition. Does not require vitamin C pairing, though it does not harm. Small amounts of haem iron consumed alongside non-haem sources also enhance non-haem absorption. |
| Sardines in tomato sauce (100g) | 2.9mg | Haem. Also provides calcium (from bones), omega 3, and vitamin D. A nutritionally dense omnivore option. | The tomato sauce provides vitamin C, enhancing any simultaneous non-haem absorption. Practical and affordable. |
The UK recommended daily iron intake is 14.8mg for premenopausal women and 8.7mg for postmenopausal women. Achieving 14.8mg requires deliberate food choices across multiple meals. A plant-based strategy reaching this target requires variety across lentils, chickpeas, seeds, fortified foods, and dark leafy greens with systematic vitamin C pairing.
Absorption Enhancers and Inhibitors: The Variables That Determine How Much Iron You Actually Absorb
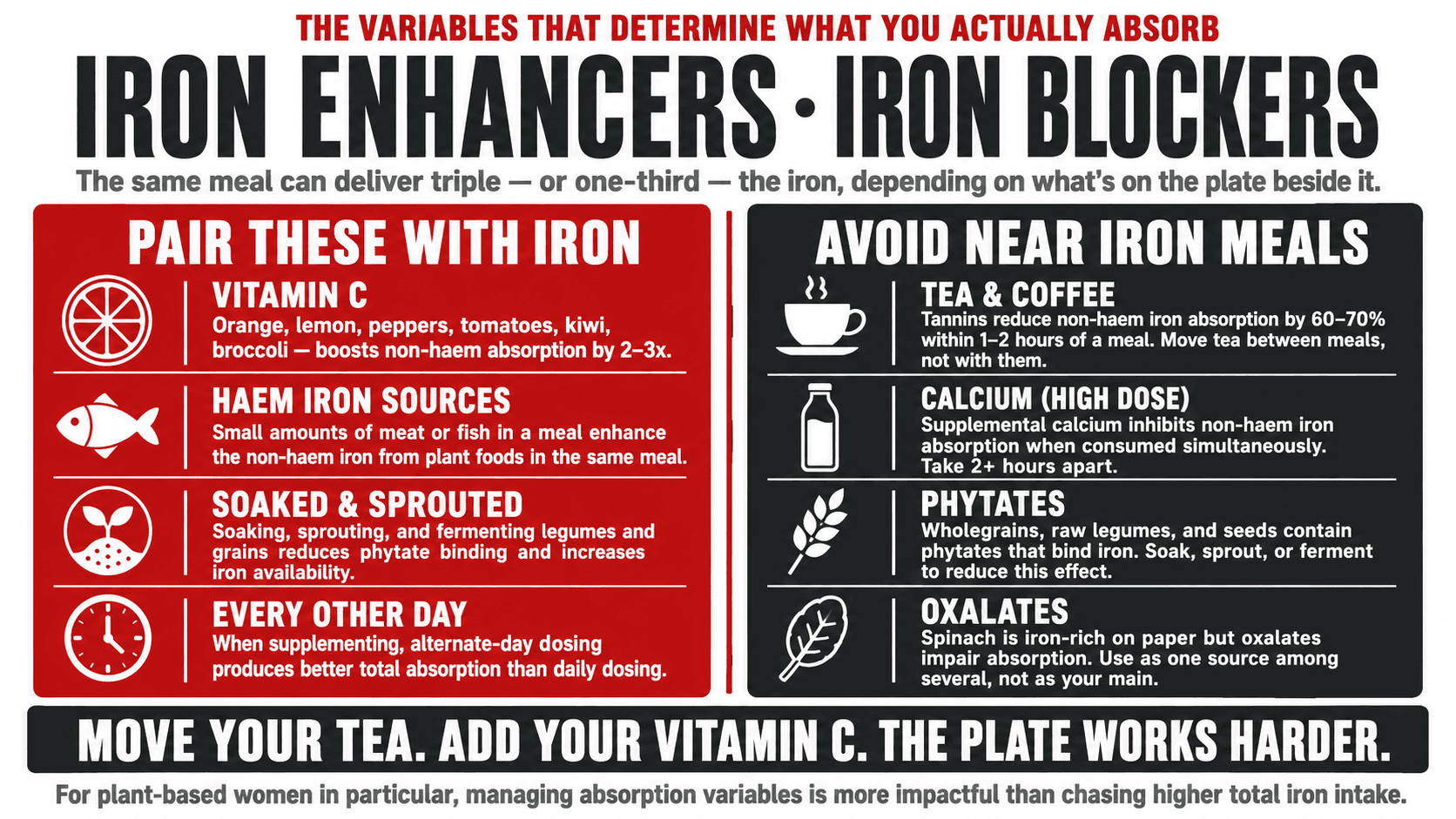
For plant-based women in particular, the total iron content of the diet is only part of the picture. The proportion of non-haem iron that is actually absorbed depends heavily on what else is present in the same meal and in the same digestive window. Managing these variables is one of the most impactful and most underused tools for improving iron status without increasing total iron intake.
Vitamin C is the most potent enhancer of non-haem iron absorption. A glass of orange juice, a squeeze of lemon, tomatoes, red peppers, broccoli, or kiwi consumed in the same meal as non-haem iron sources can increase iron absorption by two to three times. This is one of the most practically impactful nutritional pairings available and it costs nothing. Every plant-based iron source should be consumed with a vitamin C-containing food or drink (6).
Tannins in tea and coffee significantly inhibit non-haem iron absorption when consumed within one to two hours of an iron-rich meal. The degree of inhibition from a cup of tea consumed with or immediately after a meal can reduce iron absorption by 60 to 70%. This is one of the most common and most easily addressed contributors to iron deficiency in women who eat reasonable amounts of plant-based iron but drink tea or coffee habitually with or after meals.
Calcium in high doses inhibits non-haem iron absorption when consumed simultaneously. This creates a practical consideration for women taking calcium supplements: taking them at a different time of day from iron-rich meals or iron supplements reduces the inhibitory effect. The interaction is less relevant when calcium is consumed in food form alongside iron sources, but is significant for supplemental calcium.
Phytates in wholegrains, legumes, and seeds bind iron and reduce its availability for absorption. This effect can be reduced by soaking and rinsing legumes before cooking, fermenting grains, or sprouting seeds. These traditional preparation methods are effective and are worth adopting particularly for women who rely heavily on legumes and grains as their primary iron sources.
Top Tip: The single most impactful change most plant-based women can make to their iron absorption is moving tea and coffee to between meals rather than with them. Wait at least one hour after an iron-rich meal before having tea or coffee. Add a vitamin C source to every plant-based iron-containing meal. These two adjustments, applied consistently, can significantly improve functional iron status without changing total iron intake.
When Diet Is Not Enough: Iron Supplementation
There are circumstances in which dietary iron alone cannot adequately restore depleted ferritin within a reasonable timeframe, and supplementation becomes appropriate. These include ferritin below 20 to 30 mcg/L with symptoms, heavy menstrual bleeding that is consistently exceeding dietary replacement capacity, athletic training loads that substantially elevate iron requirements, or confirmed iron deficiency anaemia.
Iron supplements are available in several forms with different absorption profiles and tolerability characteristics. Ferrous sulphate is the most commonly prescribed form in the UK and has good bioavailability but frequently causes gastrointestinal side effects including constipation, nausea, and dark stools. Ferrous bisglycinate, also known as iron bisglycinate, is a chelated form with comparable absorption to ferrous sulphate at lower doses and significantly better gastrointestinal tolerability, making it the preferred supplemental form for women who struggle with the side effects of standard ferrous sulphate (7).
Dosing and timing matter considerably for iron supplementation. Taking iron on alternate days rather than daily has been shown in recent research to improve total absorption compared to daily dosing, because hepcidin, the hormone that regulates iron absorption, spikes after each iron dose and reduces subsequent absorption from a dose taken the following day. Every other day dosing allows hepcidin to return to baseline and permits more efficient absorption overall (8). Taking supplemental iron in the morning on an empty stomach or with vitamin C and away from calcium, tea, or coffee maximises the absorbed dose.
The timeline for ferritin restoration with supplementation is longer than most women expect: rebuilding ferritin from deficient to optimal levels typically requires three to six months of consistent supplementation alongside adequate dietary iron. Repeat ferritin testing at three months provides a useful progress marker.
Top Tip: If you are supplementing iron and experiencing constipation or nausea with standard ferrous sulphate, ask your pharmacist about ferrous bisglycinate as an alternative. It is available without prescription, costs slightly more, and is considerably better tolerated. Take it every other day rather than daily, in the morning before breakfast if possible, with a glass of orange juice or vitamin C supplement, and at least two hours away from calcium supplements, tea, or coffee.
Iron and Athletic Performance: What the Evidence Shows
The relationship between iron status and athletic performance is well established and clinically significant. Iron is required for haemoglobin synthesis, the oxygen-carrying capacity of the blood, and for the function of myoglobin in muscle tissue, which stores and transfers oxygen to mitochondria during exercise. Iron is also a co-factor for enzymes in the mitochondrial electron transport chain. Impaired iron status at any of these levels reduces aerobic capacity, increases the perceived effort of exercise at a given intensity, slows recovery between sessions, and reduces training adaptation (5).
Women who train consistently and find that their cardiovascular performance is chronically below what their training should produce, who feel disproportionately breathless at moderate efforts, or whose recovery between sessions seems to take longer than expected should consider ferritin as a first line investigation before adjusting training volume or intensity. The answer is frequently not the programme. It is the iron status.
The specific population of female endurance athletes, including runners, cyclists, and rowers, warrant particular attention to iron monitoring given the multiple mechanisms through which their training elevates iron requirements. A ferritin check at the beginning of a training season and after three to four months of consistent training provides a useful picture of whether dietary and supplemental strategies are keeping pace with demand.
Top Tip: Request a ferritin test before beginning a new training programme or at the start of each training season if you are a regular exerciser. A ferritin below 30 mcg/L before a high-demand training period will produce sub-optimal performance and impaired recovery regardless of how well-designed the programme is. Correct the ferritin first. The training will then produce the results it should.

The Agitate Case: What Sustained Iron Deficiency Costs a Woman
I want to be direct about what sustained iron deficiency, managed or unmanaged, costs a woman in practical terms over months and years, because I think most women significantly underestimate the impact of a nutrient deficit that is described to them as not quite anaemia.
Training that never reaches its potential. A cognitive performance ceiling that is below the actual capacity of the brain. A mood that is consistently flatter than it should be. A fatigue that makes everything, work, relationships, parenting, personal projects, feel harder than it should. These are not trivial impacts. They are the cumulative consequence of a body running on insufficient iron for its actual demands, accepted as normal because nobody told the woman in question that her ferritin of 14 was the explanation for all of it.
Immune function is also compromised by iron deficiency. Iron is required for the proliferation and maturation of immune cells, and iron-deficient women show measurably impaired immune responses to infection (3). Frequent minor illnesses, slow recovery from infections, and increased susceptibility to upper respiratory infections during periods of training are all consistent with iron-related immune suppression.
The compounding effect of addressing iron deficiency is equally striking in the other direction. Women who bring their ferritin from below 20 to above 50 through appropriate dietary and supplemental strategy consistently report what they describe as a recalibration of their normal: the return of a baseline energy level they had forgotten was possible, an improvement in training performance that their programme alone had not been able to produce, and a lifting of a low-grade mental cloud that had simply been accepted as part of life.
Top Tip: Track your energy, mood, and training performance across four to six weeks of optimised iron intake, whether through diet or supplementation. Many women notice a meaningful improvement within this window, before their next blood test confirms the change in ferritin. The improvement in subjective function is often the most motivating evidence that the intervention is working.
How I Address Iron Status in Every Female Client
Iron status is part of the baseline conversation I have with every female client before a programme begins. Not because iron deficiency is universal, but because it is common enough, and consequential enough for training performance and recovery, that it is worth assessing proactively rather than discovering reactively when results are not materialising.
The practical approach is straightforward: a symptom review, a request for ferritin alongside any existing blood test orders, and a dietary assessment that identifies whether the daily iron intake and absorption strategy are sufficient for the client's specific requirements, which vary significantly between a sedentary postmenopausal woman and a premenopausal woman training four times per week with heavy periods.
If you have been training consistently, eating reasonably well, and still feel as though something is holding your performance and energy below where they should be, iron is worth investigating before assuming the problem lies elsewhere. I work one-to-one with women online globally. The starting point is always a complete picture of what is actually happening before deciding what needs to change.
