
The Leading Cause of Death in Women That Most Women Think Belongs to Men
Cardiovascular disease in women is the leading cause of death in women in the UK, responsible for more female deaths each year than all cancers combined. This is not a new development. It has been the case for decades. And yet the persistent cultural association between heart disease and middle-aged men has created a situation in which a large proportion of women remain significantly underinformed about their own cardiovascular risk, underscreened by clinicians who do not instinctively apply cardiovascular frameworks to female patients, and undertreated when symptoms do present, partly because the symptoms of cardiac events in women differ meaningfully from the textbook male presentation (1).
I am not a cardiologist. But I am a coach who works with women across multiple decades of life, who monitors health markers as part of the coaching process, and who sees the consequences of both cardiovascular risk and cardiovascular protection in real physiological terms across years of coaching relationships. The lifestyle interventions that protect the cardiovascular system are the same interventions that build strength, support hormonal health, and sustain the energy and quality of life every woman deserves in every decade. This is not a separate health project. It is the same one.
What I want to give you in this article is what I regard as the essential cardiovascular health framework for women: why the risk profile is different from men's, why the post-menopausal transition is the most important cardiovascular inflection point in a woman's life, what the key markers to monitor are and what they mean, and what the evidence supports for protecting the heart and vascular system through lifestyle. This is information that should be part of every well woman health conversation from the age of 40 onward. Most of the time, it is not.
Why Cardiovascular Disease Is Different in Women
The narrative around cardiovascular disease has been shaped substantially by research conducted predominantly in male populations and extrapolated to women as though the biology were identical. It is not. The differences in how cardiovascular disease develops, presents, and progresses in women are clinically significant and have direct implications for how women should be assessed, screened, and supported.
Oestrogen provides meaningful cardiovascular protection during the premenopausal years through several mechanisms: it maintains endothelial function and the flexibility of blood vessel walls, promotes vasodilation, has anti-inflammatory effects, supports a favourable lipid profile by raising HDL cholesterol and reducing LDL, and reduces the tendency toward arterial stiffness. This protection is the primary reason that premenopausal women have substantially lower cardiovascular event rates than age-matched men. It is also the reason that the withdrawal of oestrogen at menopause represents the most significant cardiovascular risk transition of a woman's life (2).
After menopause, the cardiovascular risk trajectory for women accelerates sharply. LDL cholesterol rises. HDL cholesterol falls. Blood pressure increases. Inflammatory markers elevate. Visceral fat accumulates, adding its own inflammatory and metabolic cardiovascular burden. Insulin resistance worsens. Within ten years of menopause, a woman's cardiovascular risk profile approaches that of a man of the same age, having been substantially lower throughout her premenopausal decades. This convergence is not inevitable, but it is the default trajectory without active lifestyle management.
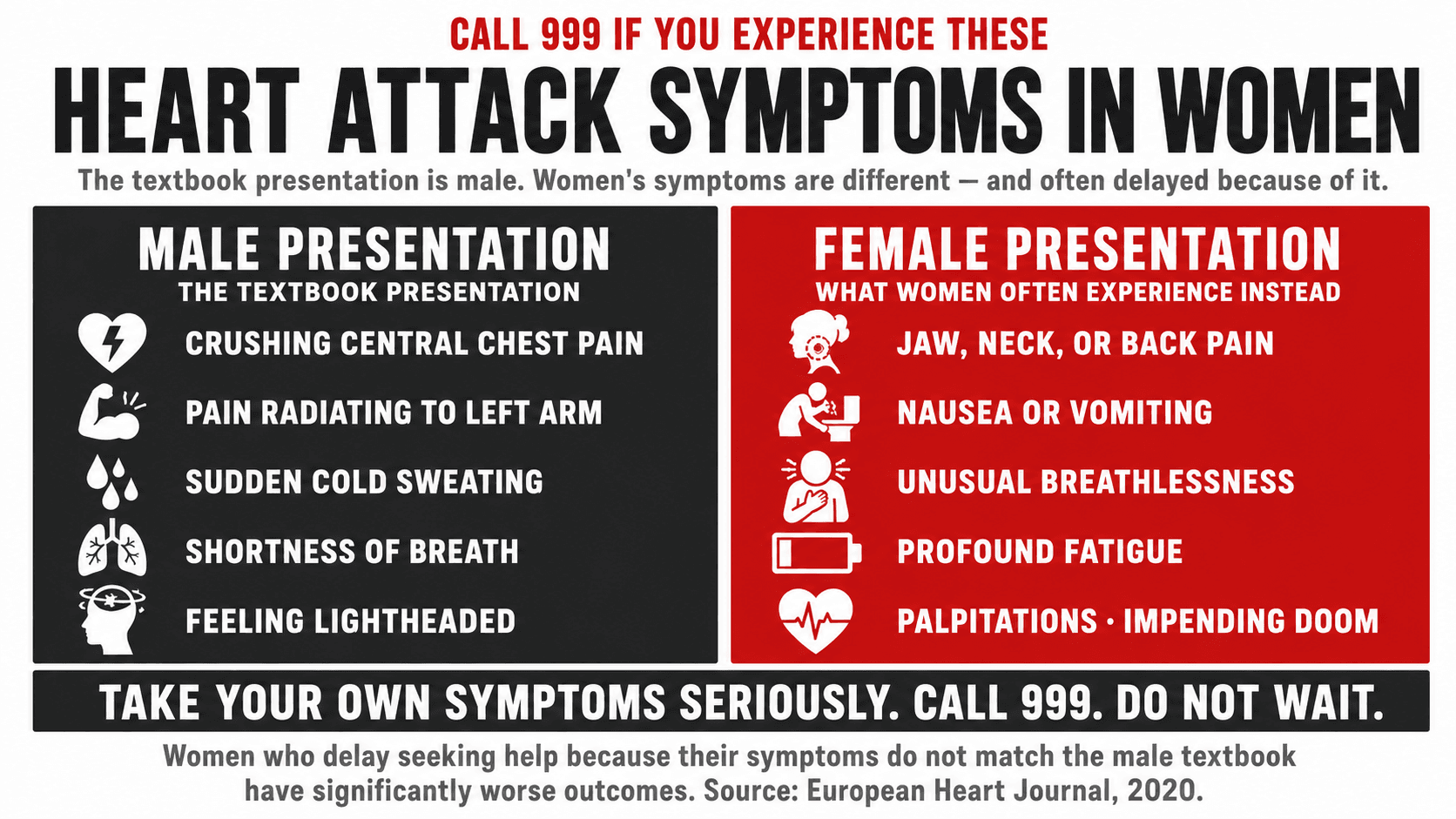
Heart attacks in women present differently than in men. The classic Hollywood heart attack, crushing central chest pain radiating to the left arm, is more characteristic of a male presentation. Women experiencing myocardial infarction are more likely to report jaw, neck, or back pain, nausea, vomiting, breathlessness, fatigue, or a sense of impending doom without dramatic chest pain. These atypical symptoms lead to delayed presentation, delayed clinical recognition, and consequently worse outcomes. A 2020 study published in the European Heart Journal found that women waited significantly longer before seeking medical attention for heart attack symptoms and were less likely to receive timely intervention than men presenting with more typical symptoms (3).
Top Tip: If you are a woman experiencing any of the following and cannot explain them: sudden jaw, neck, or back pain, unusual breathlessness, nausea or vomiting without gastrointestinal cause, profound fatigue, palpitations, or a general sense that something is seriously wrong, call 999. Do not wait to see whether the symptoms resolve. Women who delay seeking help for cardiac symptoms because they do not match the textbook male presentation have significantly worse outcomes. Take your own symptoms seriously.
The Oestrogen Protection Window and Why It Matters
Understanding oestrogen's role in cardiovascular protection is not just mechanistically interesting. It has direct practical implications for how women should approach the perimenopausal and post-menopausal years, and for the evidence around HRT and cardiovascular health.
The timing hypothesis in HRT research describes the finding that oestrogen-containing HRT started within ten years of menopause and before the age of 60 appears to confer cardiovascular protection, or at minimum does not increase cardiovascular risk, in otherwise healthy women. This window corresponds to the period before arterial atherosclerosis has substantially progressed, when the vasculature can still respond to oestrogen's anti-inflammatory and endothelial protective effects. HRT started more than ten years post-menopause, when arterial disease may already be established, carries a different risk profile (4).
The practical implication is that the post-menopausal window of maximum cardiovascular benefit for HRT is the early post-menopausal period, not the decades beyond it. This is one of the arguments for having the HRT conversation proactively around the time of menopause rather than waiting until symptoms become intolerable or until cardiovascular markers have already worsened significantly.
This is not a recommendation that every post-menopausal woman should take HRT. As I have discussed in the perimenopause and menopause articles in this series, that decision requires an individualised clinical conversation. It is a statement that the cardiovascular evidence is more favourable for HRT started early in the post-menopausal period than the legacy fear around HRT acknowledges, and that this should be part of the informed conversation.
Top Tip: If you are within five years of your last menstrual period and have not yet had a cardiovascular health baseline assessment, this is the moment to request one. Ask your GP for: fasting lipid panel (LDL, HDL, triglycerides, total cholesterol), fasting glucose and HbA1c, blood pressure measurement, and a cardiovascular risk score calculation using QRISK3. This gives you a clear picture of your cardiovascular starting position at the point when lifestyle and HRT decisions have the most influence on the trajectory.

Female-Specific Cardiovascular Risk Factors
Beyond the standard cardiovascular risk factors that apply to both sexes, women carry a set of sex-specific risk factors that are rarely included in standard cardiovascular risk conversations but that have meaningful predictive value for long-term cardiovascular outcomes.
| Risk Factor | Impact in Women | Comparison to Men | Lifestyle Response |
|---|---|---|---|
| Hypertension | Major risk factor at all ages. Women's blood pressure often lower pre-menopause due to oestrogen but rises sharply post-menopause. | Men have higher rates pre-menopause. Post-menopause the difference narrows substantially. | Resistance training and cardiovascular exercise, sodium awareness, DASH-style dietary pattern, weight management, adequate sleep. |
| Elevated LDL cholesterol | LDL rises post-menopause as oestrogen's lipid-modulating effect is lost. Small dense LDL particles are particularly atherogenic. | Men have elevated LDL earlier due to lack of oestrogen protection. Women catch up post-menopause. | Reduce saturated fat from ultra-processed sources. Increase soluble fibre: oats, lentils, beans. Exercise. Statins if clinically indicated. |
| Low HDL cholesterol | Oestrogen supports HDL synthesis. Its withdrawal reduces HDL and the reverse cholesterol transport it enables. | Men typically have lower HDL throughout life. Women's HDL advantage diminishes post-menopause. | Aerobic and resistance exercise both raise HDL. Reduce trans fats. Moderate alcohol is associated with higher HDL but risks outweigh this benefit. |
| Diabetes and insulin resistance | Women with Type 2 diabetes have 44% higher relative risk of cardiovascular events than men with Type 2 diabetes. The sex-based protection is disproportionately lost. | Diabetes elevates CVD risk in both sexes but the relative risk increase is greater in women. | Resistance training as primary insulin sensitivity intervention. Low GI nutrition. Weight management. HbA1c monitoring annually. |
| PCOS | Women with PCOS have elevated cardiovascular risk from insulin resistance, dyslipidaemia, hypertension, and chronic inflammation, independent of body weight. | No male equivalent. PCOS is an independent female-specific cardiovascular risk factor. | Resistance training. Low GI nutrition. Inositol supplementation. Regular cardiovascular screening from age 35. |
| Preeclampsia history | Women with a history of preeclampsia have two to four times the lifetime cardiovascular risk of women without this history. | No male equivalent. Preeclampsia is a strong independent predictor of future cardiovascular disease. | Lifelong cardiovascular monitoring. This history should be flagged in every GP registration and should trigger proactive screening. |
| Early menopause (before 45) | Longer duration of oestrogen withdrawal substantially elevates lifetime cardiovascular risk. Natural or surgical. | No male equivalent for this specific mechanism. | HRT is generally indicated for women with premature or early menopause specifically for cardiovascular and bone protection. Discuss with GP urgently. |
| Autoimmune conditions | Rheumatoid arthritis, lupus, and other autoimmune conditions are more common in women and carry elevated cardiovascular risk from chronic systemic inflammation. | Autoimmune prevalence is substantially higher in women. Cardiovascular risk from autoimmune inflammation is well established. | Anti-inflammatory diet. Exercise. Disease management in partnership with rheumatologist. Annual cardiovascular screening. |
Every female-specific risk factor in this table represents a missed opportunity for proactive cardiovascular screening that current clinical practice does not consistently capture. If any of these apply to you, raise them explicitly at your next GP appointment as cardiovascular risk factors, not just as reproductive or hormonal history.
What Happens to the Female Heart When the Right Lifestyle Is Absent
Cardiovascular disease does not arrive suddenly. It is built incrementally over years and decades, through the accumulation of risk factors that are not assessed, metabolic changes that are not addressed, and a lifestyle that does not provide the cardiovascular system with what it needs. The post-menopausal transition is the inflection point, but the trajectory toward or away from cardiovascular disease is set well before it.
Atherosclerosis, the process of arterial plaque accumulation that underlies the majority of heart attacks and strokes, begins silently decades before any clinical event. Endothelial dysfunction, where the arterial inner lining loses its ability to regulate blood flow and resist inflammation, is detectable in women well before menopause in those with significant risk factor burden. The arterial age of a 45-year-old woman with obesity, insulin resistance, elevated LDL, and a sedentary lifestyle may be physiologically equivalent to that of a 60-year-old woman with an active lifestyle and managed cardiovascular markers (5).
The sex-based cardiovascular protection that oestrogen provides does not protect against the consequences of decades of cardiovascular risk factor accumulation. It delays them. A woman who enters menopause with established insulin resistance, elevated LDL, hypertension, and sarcopenia does not simply lose oestrogen's protection at menopause. She enters the post-oestrogen period with an already-compromised cardiovascular baseline that then deteriorates more rapidly. The protective work happens before this transition, during the decades when the cumulative risk is building silently.
Stroke risk in women is also substantially underestimated. Women account for more than half of all stroke deaths globally, partly because women live longer and partly because female-specific risk factors including atrial fibrillation, which is more common in older women, hormonal contraceptive use in women with migraines with aura, and the cardiovascular burden of menopause are not always adequately accounted for in standard stroke risk conversations.
Top Tip: Have your blood pressure measured at least once per year from the age of 40, and at every GP appointment regardless of the reason for attending. Blood pressure measurement takes ninety seconds. Undiagnosed hypertension is one of the most common and most preventable contributors to stroke and heart disease in women. A reading of 130 over 80 or above on two separate occasions warrants discussion with your GP about management, including the lifestyle interventions that are effective before medication is required.
The Evidence-Based Lifestyle Response to Female Cardiovascular Risk
The lifestyle interventions that most effectively protect the female cardiovascular system are well established, practically accessible, and consistent across the evidence base. They are also the same interventions that address every other dimension of women's health discussed throughout this series, which is precisely why the foundations article for this series is called exactly that.
Resistance training improves cardiovascular risk markers through multiple pathways: it reduces resting blood pressure, improves lipid profiles with particular benefit to LDL and triglycerides, improves insulin sensitivity and blood glucose management, reduces visceral fat and the inflammatory burden it carries, and improves endothelial function. Research published in the British Journal of Sports Medicine demonstrated that resistance training alone, independent of aerobic exercise, produced clinically meaningful reductions in systolic and diastolic blood pressure in adults with hypertension (6). For post-menopausal women managing a rising blood pressure trend, resistance training is not a secondary recommendation to medication. It is a first-line intervention.
Cardiovascular exercise at moderate intensity improves VO2 max, reduces resting heart rate, improves cardiac output efficiency, raises HDL cholesterol, reduces triglycerides, and improves endothelial function directly. For women who have been primarily focused on resistance training, adding two to three sessions per week of moderate-intensity cardiovascular exercise, forty to sixty minutes of brisk walking, cycling, swimming, or rowing at a pace where conversation is possible but effortful, produces meaningful improvements in cardiovascular health markers beyond what resistance training alone achieves (7).
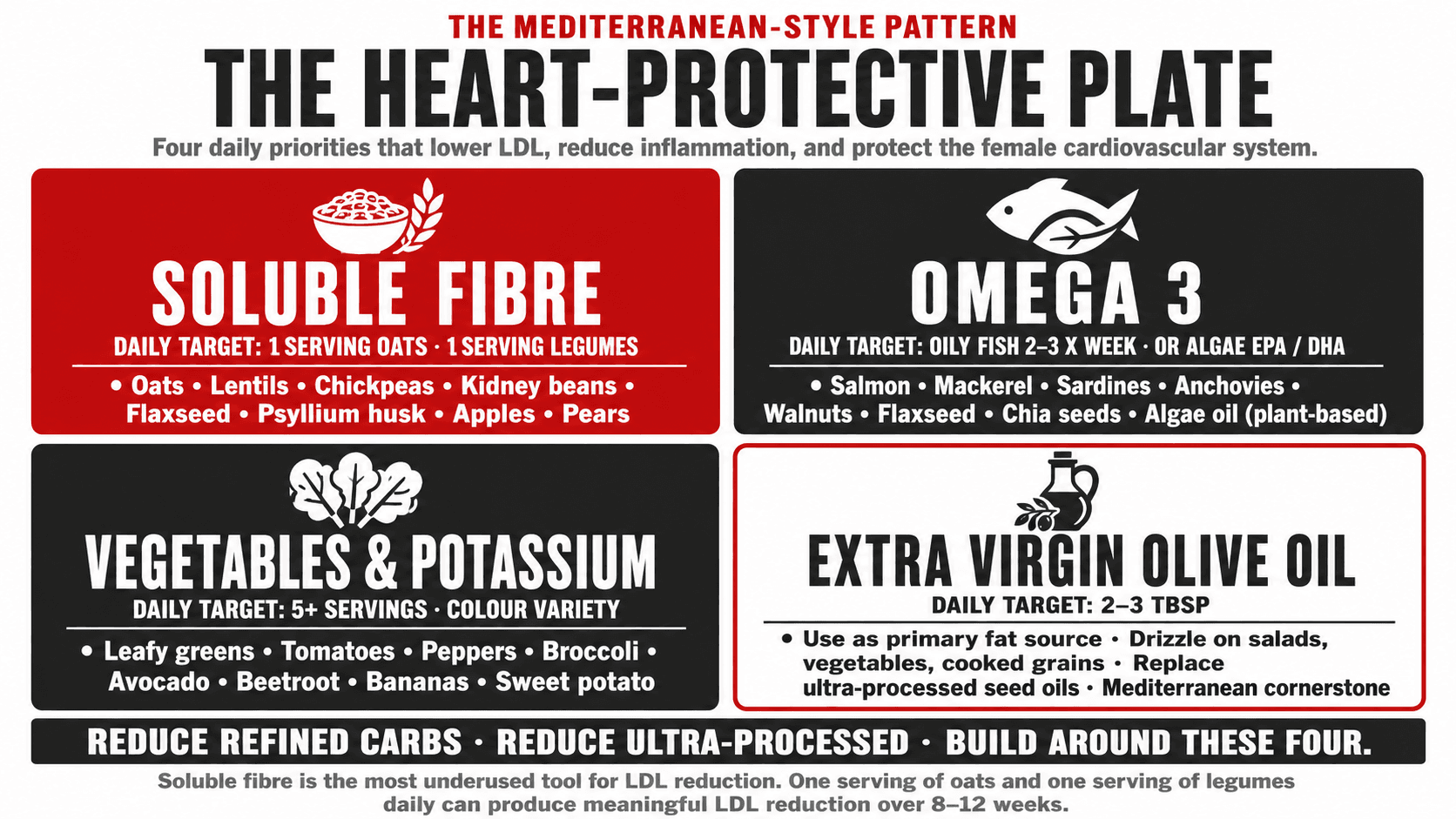
Nutrition for cardiovascular health in women is built around four evidence-based priorities: reducing LDL through soluble fibre from oats, lentils, beans, and psyllium, reducing inflammatory load through a Mediterranean-style dietary pattern rich in olive oil, fish or plant-based omega 3, vegetables, legumes, and wholegrains, managing blood glucose through limiting refined carbohydrates and ultra-processed foods, and maintaining adequate potassium through fruits and vegetables which supports blood pressure regulation. Plant-based diets are consistently associated with lower cardiovascular risk across large epidemiological studies, and women eating predominantly plant-based diets tend to have lower LDL, lower blood pressure, lower BMI, and lower inflammatory markers than omnivore comparators (8).
For omnivore women, the evidence does not require eliminating animal foods from the diet. It requires reducing the proportion of saturated fat from ultra-processed sources, increasing the proportion of plant foods, and shifting toward lean proteins, oily fish, and dairy rather than processed meats and high-fat processed products. The Mediterranean dietary pattern, which includes fish, olive oil, legumes, vegetables, wholegrains, and moderate dairy, achieves this without requiring any food group to be entirely excluded.
Top Tip: Soluble fibre is the most underused dietary tool for LDL reduction in women. Oats, lentils, chickpeas, kidney beans, flaxseed, and psyllium husk all contain beta-glucan or similar soluble fibres that bind LDL in the gut and reduce its absorption. Including one serving of oats and one serving of legumes daily, alongside adequate vegetables, can produce a meaningful reduction in LDL cholesterol over eight to twelve weeks without any medication. If your LDL is above optimal, start here before the statin conversation.
Key Cardiovascular Markers: What to Monitor and What the Numbers Mean
| Marker | Optimal Range | Concerning Level | Primary Lifestyle Response |
|---|---|---|---|
| Blood pressure | Below 120/80 mmHg | 130/80 or above on two separate occasions. Above 140/90 requires clinical intervention. | Reduce sodium. Increase potassium from fruit and vegetables. Resistance training. Cardiovascular exercise. Manage weight and stress. Discuss medication with GP if above 140/90. |
| LDL cholesterol | Below 3.0 mmol/L. Below 2.0 in those with established CVD or diabetes. | Above 3.0 mmol/L in general population. Any elevation alongside other risk factors warrants attention. | Increase soluble fibre. Reduce saturated fat from processed sources. Exercise. Consider plant sterols. Discuss statins with GP if lifestyle insufficient. |
| HDL cholesterol | Above 1.2 mmol/L for women | Below 1.0 mmol/L indicates significantly elevated cardiovascular risk. | Aerobic and resistance exercise. Reduce trans fats. Avoid smoking. Omega 3 fats. Losing excess visceral fat raises HDL. |
| Triglycerides | Below 1.7 mmol/L | Above 2.3 mmol/L significantly elevates cardiovascular and metabolic risk. | Reduce refined carbohydrates and added sugar. Reduce alcohol. Exercise. Omega 3 fatty acids. Lose excess visceral fat. |
| Fasting glucose | Below 5.6 mmol/L | 5.6 to 6.9 indicates prediabetes. Above 7.0 on two occasions indicates Type 2 diabetes. | Resistance training. Low GI dietary pattern. Post-meal walking. Weight management. Discuss HbA1c with GP if borderline. |
| HbA1c | Below 42 mmol/mol (below 6.0%) | 42 to 47 mmol/mol indicates prediabetes. Above 48 mmol/mol indicates Type 2 diabetes. | Same as fasting glucose. Three-month average. More clinically useful than a single fasting glucose for detecting trend. |
| hsCRP (inflammation) | Below 1.0 mg/L | 1.0 to 3.0 mg/L indicates moderate cardiovascular risk. Above 3.0 indicates high inflammatory risk. | Anti-inflammatory dietary pattern. Exercise. Adequate sleep. Stress management. Weight management. Address any chronic infection or autoimmune condition. |
| Waist circumference | Below 80 cm | 80 to 88 cm: increased risk. Above 88 cm: high risk regardless of total weight. | The single most clinically accessible cardiovascular risk proxy for daily monitoring. Resistance training and nutrition directly reduce visceral fat. |
Request all of these markers from your GP at age 45 to 50 as a cardiovascular baseline. Repeat every two to three years or annually if any marker is outside the optimal range. The complete picture matters more than any single result.
Smoking, Alcohol, and Oral Contraceptives: Three Cardiovascular Conversations for Women
Three specific topics warrant direct mention in the context of female cardiovascular health because they are either uniquely relevant to women or carry female-specific risk dimensions that are not always communicated clearly.
Smoking is an independent cardiovascular risk factor in both sexes, but women who smoke have a disproportionately elevated cardiovascular risk compared to male smokers at the same smoking level. The reasons include the interaction between nicotine and oestrogen metabolism, with smoking accelerating oestrogen clearance and effectively reducing the protective cardiovascular effect of endogenous oestrogen. Women who smoke and use combined oral contraceptives carry a substantially elevated risk of venous thromboembolism and stroke that is multiplicative rather than additive. This combination is one of the few absolute contraindications to combined oral contraceptive use.
Alcohol is frequently cited as having a cardiovascular protective effect at low to moderate intake, based on data showing lower cardiovascular event rates in moderate drinkers compared to abstainers in epidemiological studies. The most current evidence substantially questions the causal interpretation of this association, with Mendelian randomisation studies suggesting the protective effect is largely explained by confounding factors rather than alcohol itself. For women specifically, any cardiovascular benefit of moderate alcohol is more than offset by the elevated breast cancer risk, and the British Heart Foundation and other major cardiovascular organisations no longer advocate any level of alcohol consumption as heart-protective (9).
Combined oral contraceptives carry a small but real elevated risk of venous thromboembolism, ischaemic stroke, and myocardial infarction, with the risk being highest in women with additional cardiovascular risk factors including hypertension, migraine with aura, smoking, obesity, and a personal or family history of thrombosis. Progestogen-only contraceptives carry a substantially lower vascular risk profile. Women using combined oral contraception should be aware of these risks and should have blood pressure measured before initiation and regularly thereafter.
Top Tip: If you are using combined oral contraceptives and experience sudden severe headache, visual disturbance, one-sided weakness, speech difficulty, leg pain or swelling, or chest pain, seek emergency medical attention immediately. These are potential signs of thrombotic events that are rare but associated with combined hormonal contraceptive use. Do not wait to see whether the symptoms resolve. These are the rare but serious cardiovascular complications of this medication.
Sleep, Stress, and the Cardiovascular System in Women
Two of the most consistent and most underappreciated drivers of cardiovascular risk in women are poor sleep and chronic psychological stress. Both operate through the cortisol and sympathetic nervous system pathways that produce measurable and sustained cardiovascular effects when chronically activated.
Short sleep duration, defined as less than six hours per night, is associated with a significantly elevated risk of hypertension, Type 2 diabetes, obesity, and cardiovascular events in women. The cardiovascular consequences of chronic sleep restriction include elevated inflammatory markers, worsened insulin resistance, increased cortisol, elevated blood pressure from sustained sympathetic activation, and impaired endothelial function. Women who chronically prioritise productivity over sleep are accumulating cardiovascular risk in a way that is as physiologically meaningful as elevated LDL or physical inactivity (10).
Chronic psychological stress activates the HPA axis and sympathetic nervous system in a sustained way that produces all of the cardiovascular consequences of sleep restriction alongside its own additional burden: direct inflammatory signalling, cortisol-driven visceral fat accumulation, elevated blood pressure from sustained sympathoadrenal activation, and impaired cardiovascular recovery between stressors. Women under sustained caregiving, workplace, or financial stress carry measurably elevated cardiovascular risk markers compared to women in lower-stress circumstances, and this effect is amplified in the post-menopausal period when oestrogen's buffering of the cortisol stress response has been withdrawn.
Top Tip: Cardiovascular risk management is not complete without addressing sleep and stress. If you are managing your lipid panel, exercising regularly, and eating well but sleeping six hours per night under sustained work or caregiving pressure, you are addressing some of the cardiovascular risk factors while leaving others fully active. Seven to eight hours of sleep and some form of deliberate stress management are not soft lifestyle recommendations. They are direct cardiovascular interventions with measurable outcomes.

How Cardiovascular Health Monitoring Is Built Into My Coaching
Cardiovascular health markers are part of the baseline assessment I review with every female client from her 40s onward, and they directly inform the programme I build. A client with elevated blood pressure and high triglycerides receives a different nutritional strategy and cardiovascular exercise prescription than one with optimal markers. A client with a history of preeclampsia or PCOS receives proactive screening recommendations alongside the programme.
The lifestyle interventions described in this article are not a cardiovascular health programme separate from a body composition or performance programme. They are the same programme, built on the same foundations of resistance training, protein-led nutrition, adequate sleep, and managed stress load. The cardiovascular benefit is the systemic consequence of getting those foundations right.
If you want to understand your own cardiovascular health position clearly and build a programme that addresses it with the same precision you would apply to a body composition goal, I work one-to-one with women online globally. The heart is the most important organ you are training. It deserves to be treated that way.
