
If there is one topic that generates more confusion, more debate, and more outright misinformation than any other in the world of fat loss, it is carbohydrates. Every week, without fail, I get questions from clients, from people on social media, and from prospective clients who have been paralysed into inaction by conflicting advice about carbohydrates, insulin, and fat loss. Should I go low carb? Do carbs make you fat? Is insulin the enemy? Will eating bread stop me from losing weight? Does it matter when I eat my carbs? What about keto?
I have worked with hundreds of clients across every dietary background, from meat eaters to vegetarians to vegans, and across a spectrum of medical conditions including type 2 diabetes, type 1 diabetes, PCOS, and metabolic syndrome. I have used low carb approaches, moderate carb approaches, and higher carb approaches depending on the individual. And after all of those years and all of those transformations, I can tell you that the relationship between carbohydrates, insulin, and fat loss is far more nuanced than the internet would have you believe. This article answers the questions I hear most often, with evidence, with honesty, and without an agenda.
Do Carbohydrates Make You Fat?
No. Carbohydrates do not make you fat. Eating more calories than you burn makes you fat, regardless of whether those excess calories come from carbohydrates, fat, protein, or alcohol. This is not opinion. It is the first law of thermodynamics applied to human metabolism, and it has been confirmed by every single well-controlled metabolic ward study ever conducted (1).
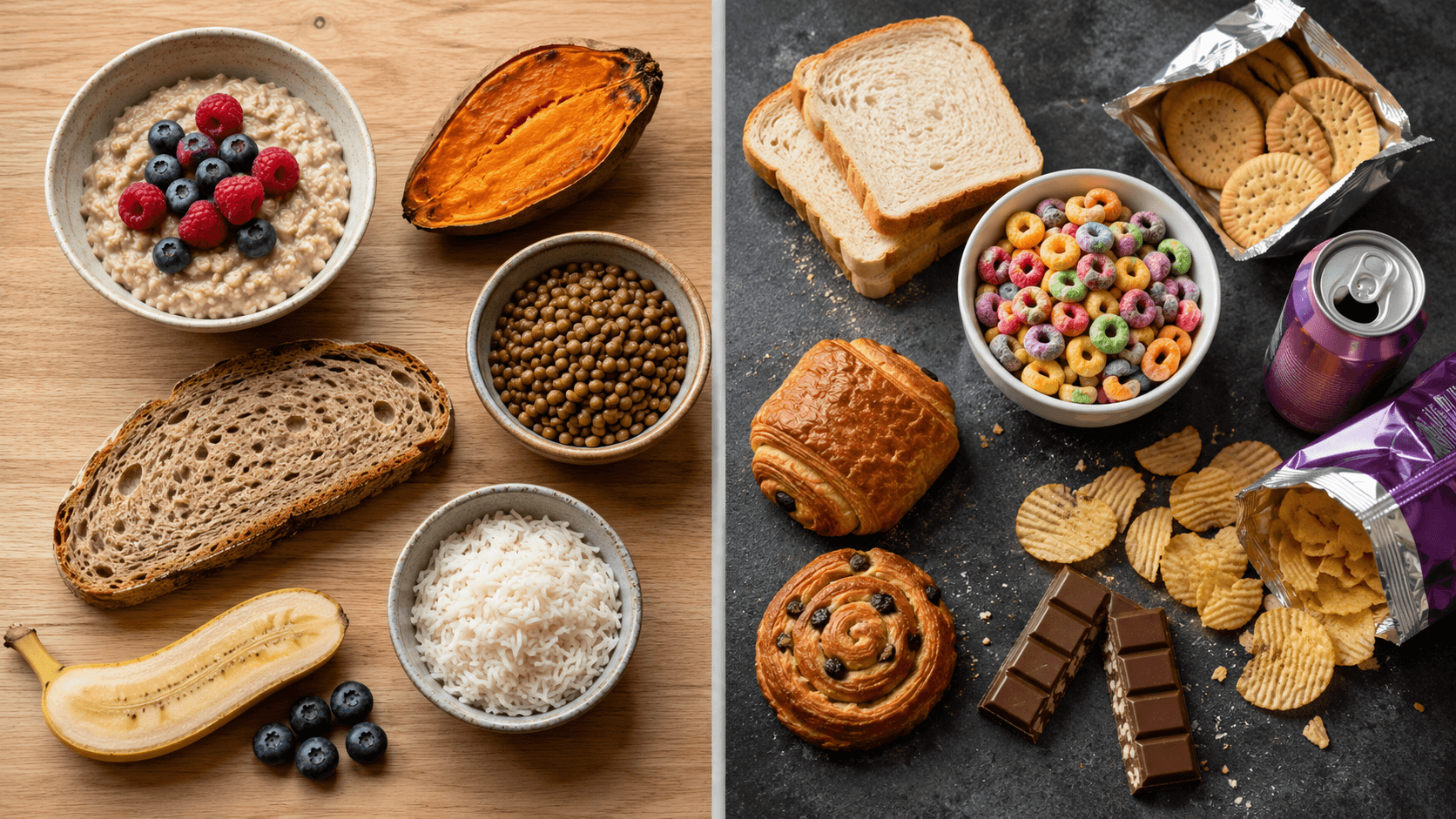
The reason carbohydrates get blamed for fat gain is that they are easy to overeat. Refined carbohydrates like white bread, biscuits, pastries, crisps, sugary cereals, and fizzy drinks are highly palatable, low in satiety, and calorie dense. They are easy to consume in large quantities without feeling full. But that is a property of highly processed foods, not of carbohydrates as a macronutrient. A bowl of lentils is a carbohydrate. A sweet potato is a carbohydrate. A portion of oats is a carbohydrate. These foods are filling, nutrient dense, and extremely difficult to overeat. The problem is not carbohydrates. The problem is the type and quantity of carbohydrates people choose.
Is Insulin the Reason I Cannot Lose Fat?
This is one of the most persistent myths in the fitness industry, and it deserves a careful answer because it contains a grain of truth wrapped in a large amount of exaggeration.
Insulin is a storage hormone. When insulin levels are elevated, lipolysis (the breakdown of stored fat) is suppressed. This is a basic physiological fact and it is the foundation of the carbohydrate-insulin model of obesity, which proposes that high carbohydrate diets drive chronically elevated insulin, which locks fat in storage and makes fat loss impossible (2). The model has some mechanistic logic, and it has been championed by prominent advocates including Gary Taubes and Dr David Ludwig.
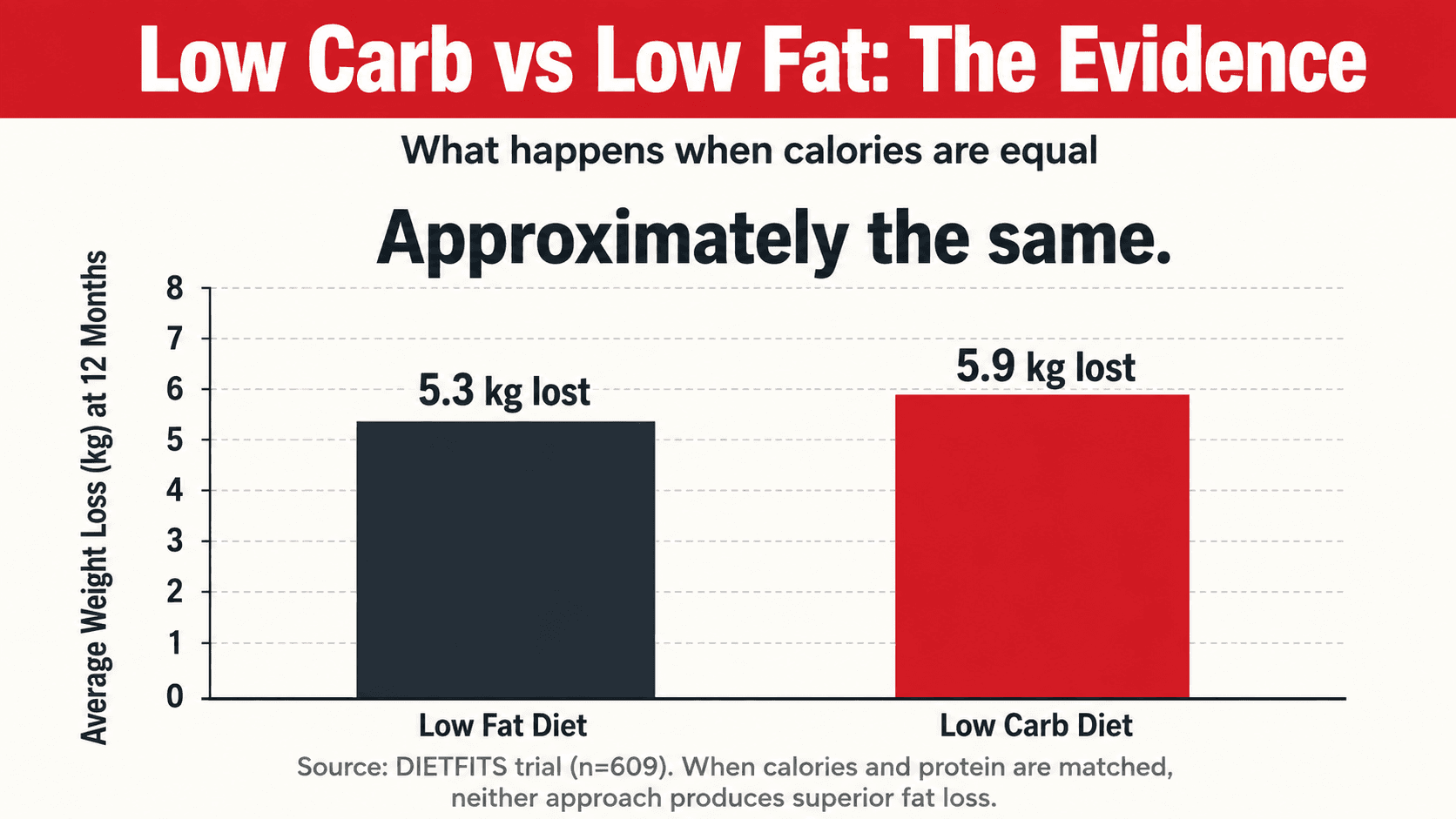
However, when this model has been tested rigorously in controlled human trials, the results have not supported it as a primary driver of obesity. The DIETFITS trial, one of the largest and most rigorous dietary intervention studies ever conducted, randomised over 600 adults to either a low fat or low carb diet for 12 months. Both groups lost similar amounts of weight (approximately 5 to 6 kilograms), and neither baseline insulin secretion nor genotype predicted which diet worked better for any individual (3). A meta-analysis of 32 controlled feeding studies, where all food was provided and calories were precisely matched, found no meaningful difference in fat loss between low carb and low fat diets when protein and calories were equated (4). If insulin were the primary driver of fat storage, low carb diets should have produced dramatically superior results. They did not.
Does this mean insulin is irrelevant? No. For individuals who are already insulin resistant, managing carbohydrate intake and insulin levels does matter, because their insulin response to carbohydrates is exaggerated, their baseline insulin is elevated, and the metabolic consequences are more pronounced. But for the general population, insulin is a normal, healthy hormone doing its job. The problem is not insulin. The problem is consuming more energy than you expend over time. Insulin is a downstream consequence of that overconsumption, not the upstream cause.
Do I Need to Go Low Carb to Lose Fat?
No. You need to be in a calorie deficit to lose fat. Whether you achieve that deficit through a low carb, moderate carb, or high carb approach is largely a matter of personal preference, adherence, and individual circumstances.
A meta-analysis of 38 randomised controlled trials comparing low carb and low fat diets found that low carb diets produced slightly more weight loss at 6 to 12 months (approximately 1.3 kilograms more), but this difference disappeared at longer time points (5). The most likely explanation for the early advantage is that low carb diets cause a rapid initial drop in water weight due to glycogen depletion (each gram of glycogen binds approximately 3 grams of water) and that higher protein intake, which often accompanies carb restriction, improves satiety and preserves muscle mass.
What the research consistently shows is that the best diet for fat loss is the one you can adhere to. If you find it easier to eat fewer calories on a lower carb approach because you feel fuller, have fewer cravings, and enjoy the foods, then lower carb will work well for you. If you train hard, love oats, rice, and sweet potatoes, and feel deprived and miserable without them, then a moderate carb approach within a calorie deficit will produce identical fat loss results. I have coached clients to outstanding transformations on both approaches. The constant is the deficit. The macronutrient split is the variable.
Should I Be Worried About Eating Carbs in the Evening?
No. The idea that carbohydrates eaten after a certain time, whether that is 6pm, 7pm, or some other arbitrary cutoff, are more likely to be stored as fat is a myth with no scientific basis. Your body does not switch from calorie burning mode to fat storage mode at a particular time of day.
A study published in the journal Obesity found that individuals who consumed the majority of their daily carbohydrates at dinner actually lost more weight and body fat than those who spread their carbohydrates evenly throughout the day, and also showed greater improvements in satiety hormones and inflammatory markers (6). The total amount of carbohydrates you eat over the course of 24 hours matters. The exact time you eat them does not, in any meaningful metabolic sense.
There is, however, a practical reason why some people benefit from reducing carbohydrates in the evening, and it has nothing to do with metabolism. It has to do with behaviour. For many people, the evening is when mindless snacking happens. Biscuits, crisps, toast, cereal, chocolate. If restricting carbohydrates after dinner helps you eliminate 300 to 500 calories of evening snacking, then it works as a behavioural strategy, not because of any metabolic magic. I use this approach with some clients because it is effective for controlling total intake, not because evening carbohydrates are inherently fattening.
How Many Carbohydrates Should I Eat for Fat Loss?
There is no single answer to this question because the right amount depends on your total calorie budget, your training volume, your body composition goals, your insulin sensitivity, and your personal preferences. But I can give you a practical framework that works for the vast majority of clients I coach.
I set protein first, always. For fat loss, that means 1.8 to 2.2 grams per kilogram of bodyweight per day. I then set a fat minimum of 0.7 to 1.0 grams per kilogram to support hormonal health and essential fatty acid needs. The remaining calories come from carbohydrates. For most people in a moderate calorie deficit, this results in a carbohydrate intake of roughly 2 to 4 grams per kilogram of bodyweight per day. That is enough to fuel your training, support your recovery, keep your fibre intake high, and maintain the variety and flexibility that makes your diet sustainable.
For clients with insulin resistance, PCOS, type 2 diabetes, or metabolic syndrome, I often start at the lower end of that range and prioritise lower glycemic, fibre-rich sources like oats, lentils, chickpeas, sweet potatoes, quinoa, and legumes. For clients who are lean, train intensely, and have good insulin sensitivity, I keep carbohydrates higher because they fuel performance, support recovery, and there is no physiological reason to restrict them. For vegetarian and vegan clients, carbohydrate sources like legumes, beans, lentils, and whole grains are also their primary protein sources, so the interplay between macronutrients requires careful planning to ensure both protein and carbohydrate targets are met.
Are All Carbohydrates the Same?
Absolutely not, and this is one of the most important distinctions in nutrition that gets lost in the low carb versus high carb debate. Treating all carbohydrates as a single category is like treating all fats as a single category. The biological effects of a bowl of lentils and a can of fizzy drink could not be more different, even though both are classified as carbohydrates.
Whole, minimally processed carbohydrate sources like oats, sweet potatoes, legumes, beans, whole grains, vegetables, and most fruits are digested slowly, produce a moderate blood glucose and insulin response, provide fibre, vitamins, minerals, and phytonutrients, and are highly satiating. They are some of the most health-promoting foods on the planet. Populations that consume diets rich in these foods, such as traditional Mediterranean, Okinawan, and Blue Zone diets, have among the lowest rates of obesity, type 2 diabetes, and cardiovascular disease in the world (7).
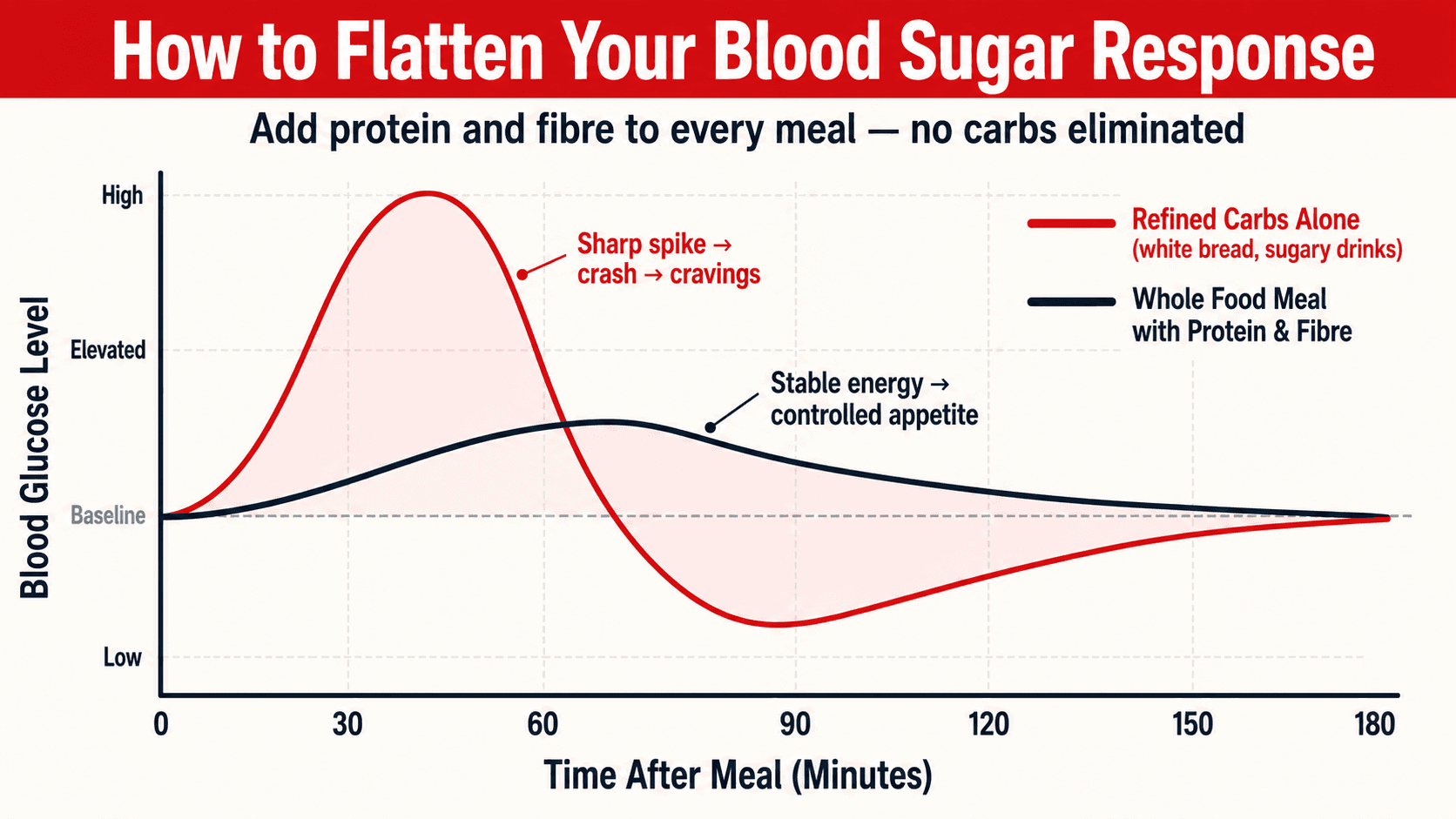
Ultra-processed carbohydrates like white bread, pastries, sugary cereals, sweets, biscuits, and sugar-sweetened beverages are digested rapidly, produce sharp blood glucose and insulin spikes followed by crashes, contain minimal fibre or micronutrients, and are easy to overconsume. A landmark study by Kevin Hall at the National Institutes of Health found that when people were given unlimited access to ultra-processed food, they spontaneously consumed 500 more calories per day compared to when they were given whole, minimally processed food, despite both diets being matched for available macronutrients (8). That 500 calorie difference was not driven by carbohydrates per se. It was driven by the processing.
When I build nutrition plans for my clients, I do not restrict carbohydrates as a category. I prioritise whole food carbohydrate sources and minimise ultra-processed ones. The result is a diet that is naturally lower in glycemic load, higher in fibre, more satiating, and far more conducive to fat loss, without the psychological burden of carbohydrate restriction.
Does Eating Carbohydrates Stop Me From Burning Fat?
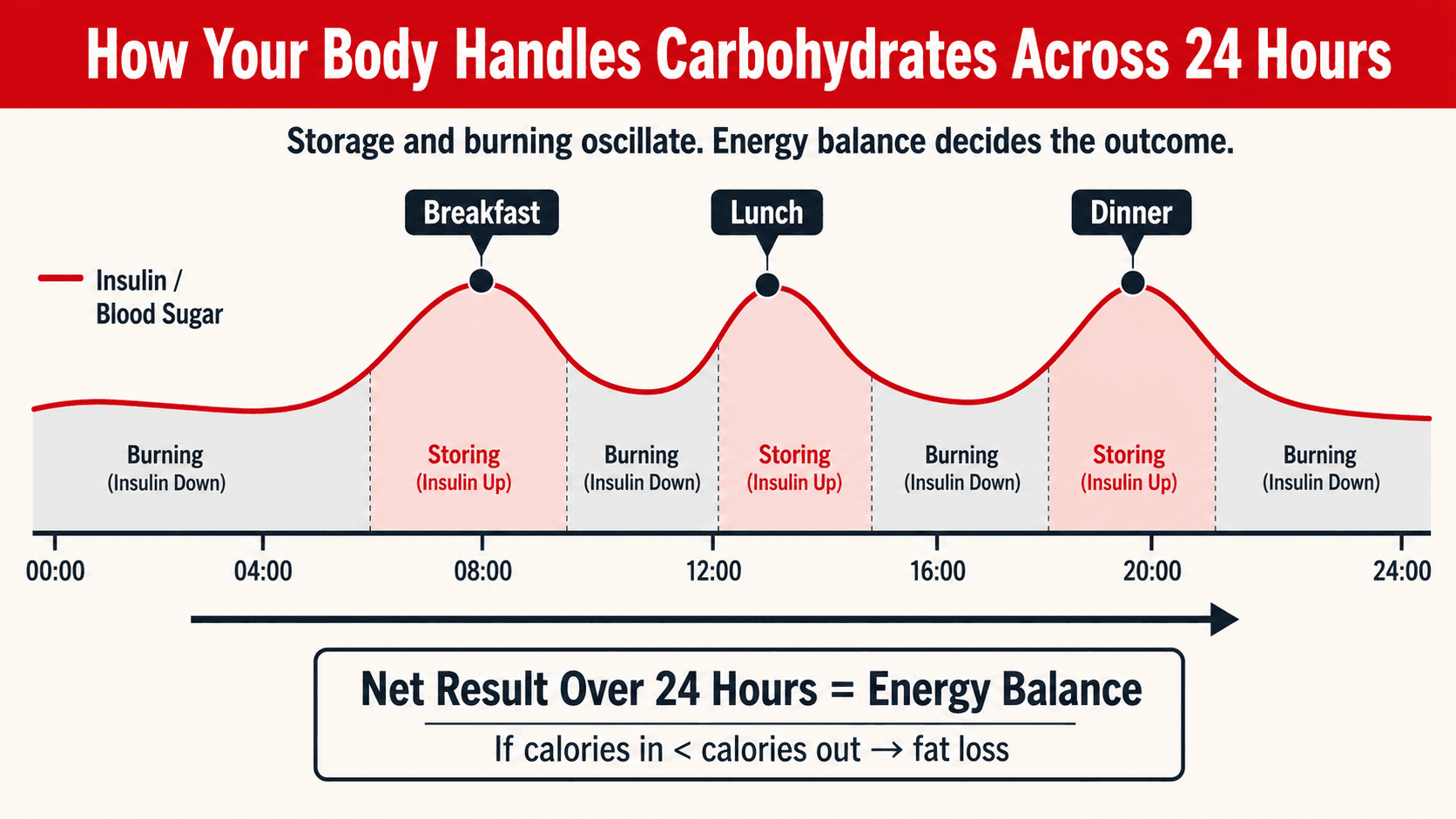
This question comes from a misunderstanding of how fat oxidation works. It is true that when you eat carbohydrates, insulin rises, and while insulin is elevated, fat oxidation is temporarily suppressed. Your body preferentially burns the glucose you have just consumed. This is normal physiology. But it does not mean you are not losing body fat.
Fat loss is determined by your energy balance over 24 hours, not by whether you are burning fat at any given moment during the day. When you eat, you store some energy. Between meals and overnight, you burn stored energy, including fat. If your total energy intake is less than your total energy expenditure over the course of the day, you lose fat. The transient rise in insulin after a meal does not prevent this. It is simply your body's normal mechanism for dealing with incoming fuel (9).
The only scenario where carbohydrate-driven insulin becomes a genuine barrier to fat loss is in clinical insulin resistance, where baseline insulin levels are chronically elevated and the normal oscillation between fed-state storage and fasted-state burning is impaired. For these individuals, managing carbohydrate type, quantity, and timing becomes more important. For everyone else, eating carbohydrates within a calorie deficit does not prevent fat loss. Your body is perfectly capable of burning fat and eating carbohydrates in the same 24 hour period.
Should I Time My Carbohydrates Around Training?
For most people training for body composition, nutrient timing is a minor detail rather than a major priority. Your total daily intake of calories, protein, and carbohydrates matters far more than exactly when you eat them. However, there is evidence that carbohydrate timing can offer a small but meaningful advantage, particularly for people training intensely or managing insulin resistance.
Your muscles are most insulin sensitive during and immediately after exercise. GLUT4 transporters, which shuttle glucose into muscle cells, are upregulated by muscle contraction independently of insulin (10). This means that carbohydrates consumed around your training sessions are preferentially directed into muscle glycogen stores rather than fat stores, even in individuals with some degree of insulin resistance. For this reason, I often programme the majority of my clients' daily carbohydrate intake in the meals before and after training. This is not about magic. It is about taking advantage of the window where your body handles carbohydrates most efficiently.
For clients with insulin resistance, PCOS, or type 2 diabetes, this timing strategy becomes more valuable because it allows them to consume adequate carbohydrates to fuel their training while minimising the insulin burden during the rest of the day when their cells are less responsive. For healthy, insulin-sensitive individuals who are training primarily for body composition, the benefit is smaller but still worth implementing because it costs nothing and may slightly improve nutrient partitioning.
What About Keto? Is It Better for Fat Loss?
Ketogenic diets, which restrict carbohydrates to typically below 20 to 50 grams per day, forcing the body to rely primarily on fat and ketone bodies for fuel, are not inherently superior for fat loss when calories are matched. They are simply another way to create a calorie deficit.
The initial weight loss on a ketogenic diet is often dramatic, frequently 3 to 5 kilograms in the first week. But the majority of this is water loss from glycogen depletion, not fat loss. When studies control for this initial water loss and measure actual body fat change over weeks and months, the difference between keto and other dietary approaches is minimal (4). A meta-analysis of low carb diets in individuals with obesity found significant weight loss at 3 to 8 months but no meaningful difference from balanced diets at 10 months or beyond (11). The advantage appears to be short-term and largely driven by adherence, protein intake, and appetite suppression rather than any unique metabolic mechanism of ketosis itself.
Some people thrive on keto. They find it easy to adhere to, they enjoy the foods, and they feel satisfied. For those individuals, it works well. But many others find it unsustainable, socially restrictive, and incompatible with the foods they enjoy. It eliminates most fruits, all grains, all legumes, and all starchy vegetables, which are among the most nutrient-dense and health-promoting food groups available. For my vegetarian and vegan clients, keto is practically impossible because the primary plant-based protein sources, including lentils, chickpeas, beans, and tofu, all contain meaningful carbohydrates. I rarely recommend ketogenic diets for long-term use. I do occasionally use short-term low-carb kickstart phases for insulin-resistant clients, but always with a plan to reintroduce carbohydrates progressively as their insulin sensitivity improves.
What Is the Single Most Important Thing to Understand About Carbs and Fat Loss?
That carbohydrates are a tool, not a villain. They are a macronutrient that provides energy, fuels your training, supports your recovery, feeds your gut microbiome, and makes your diet enjoyable and sustainable. The problem has never been carbohydrates themselves. It has been the overconsumption of highly processed, calorie-dense, nutrient-poor carbohydrate sources within a lifestyle that does not expend enough energy to accommodate them.
If you eat whole food carbohydrate sources, control your portions, maintain a calorie deficit, hit your protein target, train with weights, walk daily, and sleep well, carbohydrates will not prevent your fat loss. They will support it. The clients who achieve the best results with me are not the ones who fear carbohydrates. They are the ones who understand how to use them intelligently.
Top Tips: Carbohydrates, Insulin, and Fat Loss
Set your calorie deficit first. Your macronutrient split is secondary. No amount of carbohydrate manipulation will produce fat loss if you are not in a sustained energy deficit. Get your calories right, set your protein at 1.8 to 2.2 grams per kilogram, set your fat minimum, and fill the remaining calories with carbohydrates. The deficit drives the result. The carbohydrate amount is a preference.
Choose whole food carbohydrate sources for 80 percent or more of your intake. Oats, sweet potatoes, basmati rice, quinoa, lentils, chickpeas, beans, whole fruits, and vegetables. These sources are filling, nutrient dense, lower glycemic, and high in fibre. They support stable blood sugar, controlled appetite, and consistent energy. Save the refined stuff for occasional flexibility, not daily consumption.
Do not fear carbohydrates in the evening. Your metabolism does not shut down at sunset. If evening carbohydrates fit your calorie target and your macros, eat them. If restricting evening carbohydrates helps you avoid mindless snacking, use it as a behavioural strategy. But do not believe it is metabolically necessary.
If you are insulin resistant, manage carb type and timing before reducing total carbs. Switch from refined to whole food sources, add fibre to every meal, eat protein before carbohydrates, walk after meals, and front-load your carbs around training. These changes improve your glycemic response dramatically without the need for extreme restriction.
Stop looking for the perfect macronutrient ratio. It does not exist. The DIETFITS trial, the A to Z trial, and multiple systematic reviews all confirm the same finding: no single macronutrient ratio produces superior fat loss when calories and protein are matched (3, 12). Find the split that you enjoy, that fuels your training, and that you can sustain for months. That is the right ratio for you.
Eat protein and fibre at every meal to blunt the glycemic response. Adding protein and fibre to a carbohydrate-containing meal slows digestion, reduces the blood glucose spike, and produces a more controlled insulin response. This is one of the simplest and most effective strategies for improving how your body handles carbohydrates, and it requires no food elimination whatsoever.
Judge your diet by results, not by ideology. If your body fat is decreasing, your waist circumference is shrinking, your energy is good, your training is strong, and your blood work is improving, your carbohydrate intake is fine. Do not let internet arguments about insulin convince you to change something that is already working.
The Bottom Line
Carbohydrates are not the enemy of fat loss. They never were. The enemy is overconsumption, under-movement, and the relentless misinformation that turns a straightforward nutritional tool into a source of fear, confusion, and paralysis. Eat whole food carbohydrates, control your portions, train hard, walk daily, sleep well, and stay in a deficit. If you have insulin resistance, be smarter about which carbohydrates you choose and when you eat them. If you do not, stop worrying and eat the sweet potato.
If you want a personalised nutrition plan that takes the guesswork out of carbohydrates, insulin, and fat loss, and that is built around your body, your health, your training, and your dietary preferences, get in touch. I work one-to-one with clients online globally. Whether you eat meat, are vegetarian, vegan, or anywhere in between, whether you are managing diabetes, PCOS, or simply want to get leaner and healthier, I will build a plan that works. No fads. No fear. Just evidence, precision, and results.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- Hall KD, Guo J. Obesity energetics: body weight regulation and the effects of diet composition. Gastroenterology. 2017; 152(7): 1718-1727.
- Ludwig DS, Ebbeling CB. The carbohydrate-insulin model of obesity: beyond calories in, calories out. JAMA Internal Medicine. 2018; 178(8): 1098-1103.
- Gardner CD, Trepanowski JF, Del Gobbo LC, et al. Effect of low-fat vs low-carbohydrate diet on 12-month weight loss in overweight adults and the association with genotype pattern or insulin secretion: the DIETFITS randomized clinical trial. JAMA. 2018; 319(7): 667-679.
- Hall KD, Bemis T, Brychta R, et al. Calorie for calorie, dietary fat restriction results in more body fat loss than carbohydrate restriction in people with obesity. Cell Metabolism. 2015; 22(3): 427-436.
- Chawla S, Tessarolo Silva F, Amaral Medeiros S, Mekary RA, Radenkovic D. The effect of low-fat and low-carbohydrate diets on weight loss and lipid levels: a systematic review and meta-analysis. Nutrients. 2020; 12(12): 3774.
- Sofer S, Eliraz A, Kaplan S, et al. Greater weight loss and hormonal changes after 6 months diet with carbohydrates eaten mostly at dinner. Obesity. 2011; 19(10): 2006-2014.
- Buettner D, Skemp S. Blue Zones: lessons from the world's longest lived. American Journal of Lifestyle Medicine. 2016; 10(5): 318-321.
- Hall KD, Ayuketah A, Brychta R, et al. Ultra-processed diets cause excess calorie intake and weight gain: an inpatient randomized controlled trial of ad libitum food intake. Cell Metabolism. 2019; 30(1): 67-77.
- Frayn KN. Metabolic Regulation: A Human Perspective. 3rd ed. Oxford: Wiley-Blackwell; 2010.
- Richter EA, Hargreaves M. Exercise, GLUT4, and skeletal muscle glucose uptake. Physiological Reviews. 2013; 93(3): 993-1017.
- Silverii GA, Botarelli L, Dicembrini I, et al. Effectiveness of low-carbohydrate diets for long-term weight loss in obese individuals: a meta-analysis of randomized controlled trials. Diabetes, Obesity and Metabolism. 2022; 24(8): 1458-1468.
- Sacks FM, Bray GA, Carey VJ, et al. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. New England Journal of Medicine. 2009; 360(9): 859-873.
