
The Framework Most Women Have Never Been Given
The foundations of women's health are not complicated, but they are consistently misrepresented. For most of the women who come to me, the years before they walked through my door were spent fighting their bodies rather than understanding them. Chronic dieting. Excessive cardio. Frustrating plateaus. An endless cycle of restriction and rebound that left them feeling like the problem was them. It was not. The problem was the framework they had been given, or more accurately, the one they had never been given.
I have seen the same pattern play out repeatedly. Women who work incredibly hard, who are disciplined and determined, and who still cannot achieve the results they want because nobody has ever explained how the female body actually works, what it needs, and crucially, what it does not respond well to. The standard advice, eat less and move more, is a blunt instrument applied to a system that requires considerably more precision.
This article is the foundation piece for every article I write on women's health. It lays out the five non-negotiable pillars of a healthy, strong female body, explains why the female body is not a smaller version of the male body and why the approach must reflect that, and gives you a clear starting point for building a health strategy that actually works with your physiology rather than against it.
Whether you are 30 and feeling the first shifts in how your body responds to training and food, 45 and navigating the perimenopausal transition, or 55 and rebuilding after menopause, these pillars are the foundation. Everything else sits on top of them.
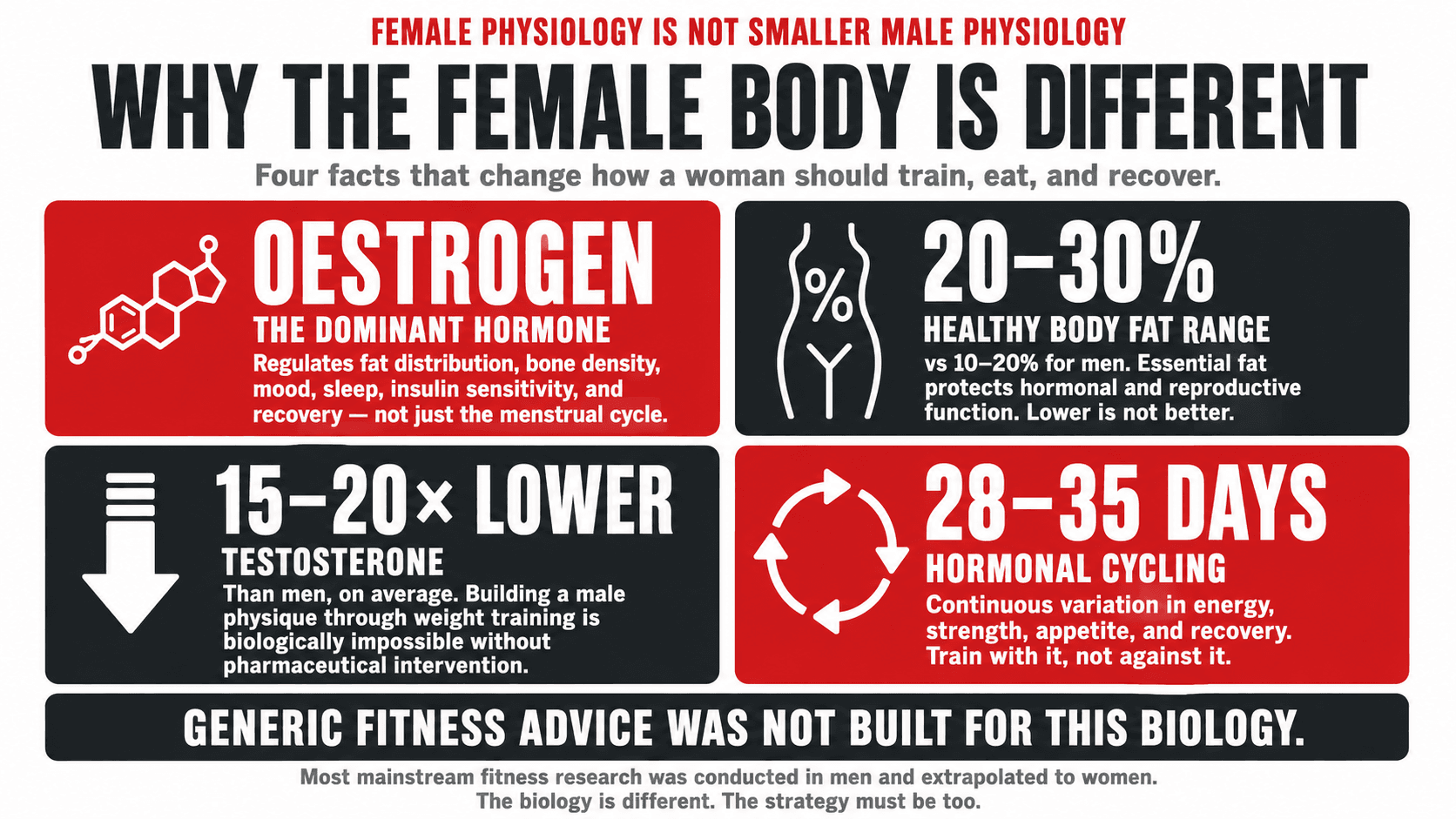
Why the Female Body Is Not a Smaller Version of the Male Body
This sounds obvious when stated plainly, yet most mainstream fitness and nutrition advice has been built on research conducted primarily in men, extrapolated to women as though the biology were identical. It is not. The differences are significant, clinically meaningful, and practically important for how women should train and eat.
Oestrogen is the dominant sex hormone in women of reproductive age and it does far more than regulate the menstrual cycle. Oestrogen influences fat distribution, bone density, cardiovascular health, insulin sensitivity, mood, sleep architecture, and recovery from exercise. Its fluctuation across the menstrual cycle creates a metabolic and physiological environment that changes week by week, affecting everything from strength levels to appetite to how efficiently the body burns fat. Women who do not account for this cycling are operating with one hand tied behind their back (1).
Women carry a higher baseline body fat percentage than men for entirely valid physiological reasons. The female body requires a minimum level of essential fat to support hormonal function, reproductive health, and the structural protection of internal organs. Aiming for male body fat standards is not only unrealistic but physiologically inappropriate and potentially harmful. The healthy body fat range for women is 20 to 30% for general health, compared to 10 to 20% for men (2). This is not a deficit. It is biology.
Women have substantially lower testosterone levels than men, approximately 15 to 20 times lower on average. This single fact dismantles the fear that weight training will produce a male physique. The hormonal environment required to build the kind of muscle mass that many women worry about simply does not exist in the female body without pharmaceutical intervention. What resistance training does produce in women is a leaner, stronger, more metabolically active physique that is the opposite of bulky.
The practical implication of all of this is that women need a training and nutrition strategy built specifically for female physiology. Not a watered-down male programme. Not a generic calorie deficit. A strategy that accounts for hormonal cycling, that prioritises the right kind of training for the female body, that provides the right nutrients in the right amounts, and that treats recovery as a non-negotiable rather than a luxury.
Top Tip
The BMI scale and the number on the scales are the two least useful tools for assessing a woman's health and body composition. A woman who weighs the same as she did five years ago but has replaced three kilograms of fat with three kilograms of muscle is in a profoundly different and better physiological position. Focus on how you feel, how you perform, your waist measurement, and your energy levels. These tell a more accurate story.
Body Composition Reference Ranges for Women
| Category | Body Fat % (Women) | Waist Circumference | Health Implications |
|---|---|---|---|
| Essential Fat | 10 to 13% | Not a useful marker at this level | Required for hormonal function and organ protection. Below this level: amenorrhoea, bone loss, hormonal shutdown. |
| Athletic | 14 to 20% | Below 80cm: lower risk | High performance physique. Achievable and sustainable with consistent resistance training and good nutrition. |
| Fitness | 21 to 24% | Below 80cm: lower risk | Excellent health profile. Optimal zone for most women balancing health, energy, and sustainability. |
| Acceptable | 25 to 31% | 80 to 88cm: increased risk | Within healthy range. Health risk increases toward the upper end, particularly with central adiposity. |
| Overweight | 32 to 39% | 80 to 88cm: increased risk | Elevated metabolic, cardiovascular, and hormonal risk. Lifestyle intervention is strongly indicated. |
| Obese | 40% and above | Above 88cm: high risk | Significantly elevated risk across cardiovascular, metabolic, hormonal, and musculoskeletal systems. Immediate lifestyle intervention warranted. |
Body fat percentage measured by DEXA or validated skinfold assessment is more clinically useful than BMI for women. Waist circumference above 80cm indicates increased health risk for women, above 88cm indicates high risk. These are the two measurements worth tracking.
The Five Pillars of Women's Health
Everything I build for female clients is structured around five non-negotiable pillars. These are not independent of one another. They interact, reinforce one another, and when any one of them is neglected, the others are undermined. Understanding each one, and why it matters specifically for the female body, is the starting point for any meaningful change.
THE 5 PILLARS OF WOMEN'S HEALTH
01
Body Composition
Not just weight. The ratio of muscle to fat. Waist circumference over BMI. DEXA or skinfold assessment. The foundation metric.
02
Resistance Training
The most important exercise. Builds and preserves muscle. Protects bone density. Improves insulin sensitivity. 3 to 4 sessions per week.
03
Nutrition Quality
Protein first. Every meal. 1.6 to 2g per kg bodyweight. Fibre for blood sugar stability. Iron, calcium, vitamin D. Not undereating. Fuelling.
04
Hormonal Health
Understand your cycle. Oestrogen, progesterone. Cortisol management. Sleep as hormonal medicine. Periodic health screening.
05
Recovery
7 to 8 hours of sleep. Stress management. Deload weeks in training. Post-training nutrition. Non-negotiable, not optional.
Neglect any one of these five pillars and the others are compromised. Optimise all five simultaneously and the results compound in every direction.
Pillar One: Body Composition
Body composition is the single most important measurement tool for women's health, and it is the one most women have never had properly assessed. Weight is a crude and often misleading metric. A woman who weighs 70kg with 35% body fat is in a fundamentally different health position to a woman who weighs 70kg with 22% body fat. The scale cannot tell them apart. Body fat percentage, measured accurately through DEXA scanning or calibrated skinfold assessment, tells you something the scales never can.
Waist circumference is the second measurement that matters. Central adiposity, the accumulation of visceral fat around the abdomen and organs, carries the most significant health risk for women, particularly after menopause when oestrogen-driven protective fat distribution patterns shift. A waist circumference above 80cm indicates increased health risk for women. Above 88cm indicates high risk, regardless of total body weight (3).
The goal is not the lowest possible number on the scale. The goal is the highest ratio of muscle to fat that is sustainable and consistent with your life, your health, and your energy levels. That goal requires building or preserving muscle, which requires resistance training and adequate protein. Not restriction. Not more cardio.
Top Tip
Measure your waist circumference once per month at the narrowest point, first thing in the morning before eating, using a tape measure. This single measurement gives you more clinically relevant information about your metabolic health trajectory than daily weighing. Target a measurement below 80cm for the lowest health risk category.

Pillar Two: Resistance Training
Resistance training is the most important physical intervention available to women at every stage of life, and it is the one most consistently avoided, underused, or approached with insufficient intensity to produce meaningful results. The fear of becoming bulky is the most common reason women give for avoiding weights. I address this directly and in detail in a dedicated article in this series. The short answer is that the hormonal environment of the female body makes this outcome effectively impossible without pharmaceutical assistance.
What resistance training actually does to a woman's body is build and preserve muscle tissue, which in turn raises the resting metabolic rate, making fat loss more effective and more sustainable. It increases bone density through mechanical loading, which is the most evidence-supported intervention for preventing osteoporosis. It improves insulin sensitivity, which directly reduces the risk of Type 2 diabetes and PCOS symptom severity. It improves cardiovascular markers. It supports psychological health through measurable improvements in self-efficacy, mood, and body image. And it preserves physical capability and functional independence into old age (4).
For most women, three to four resistance training sessions per week of forty-five to sixty minutes, structured around compound movements that recruit the largest muscle groups, is sufficient to produce significant and sustained improvements in body composition, metabolic health, and physical performance. The most important exercises are the ones that load the most muscle tissue simultaneously: squats, deadlifts, hip hinges, rows, presses, and carries.
Top Tip
The single most common reason women do not get results from resistance training is insufficient effort. Using weights that are genuinely challenging, where the last two to three repetitions of each set require real effort, is what drives adaptation. If every session feels comfortable, the stimulus is not sufficient to produce change. Progressive overload, gradually increasing the load or volume over time, is the mechanism through which training produces results.

Pillar Three: Nutrition Quality
The most common nutritional mistake I see in women who come to me having tried everything is undereating. Chronic calorie restriction, particularly the restriction of protein and dietary fat, is the fastest route to a slower metabolism, lost muscle mass, hormonal disruption, and a body that becomes progressively harder to change. The female body interprets sustained calorie restriction as a survival threat and responds by reducing metabolic rate, increasing appetite, and shifting toward fat storage.
Protein is the most important macronutrient for women and the most consistently insufficient in women's diets. The evidence supports a target of 1.6 to 2.2 grams of protein per kilogram of bodyweight per day for women engaged in resistance training and pursuing body composition improvements (5). Protein supports muscle protein synthesis, stabilises blood glucose by slowing gastric emptying, supports satiety more effectively than any other macronutrient, and is essential for hormonal production, immune function, and tissue repair.
For plant-based women, achieving adequate protein requires deliberate planning but is entirely achievable. Tofu, tempeh, seitan, soy protein isolate, pea protein, lentils, chickpeas, black beans, edamame, and high-protein grains such as quinoa are the building blocks of a plant-based protein strategy. Spreading protein across three to four meals throughout the day, with each meal containing a meaningful protein source, is both practical and effective.
Carbohydrate quality rather than carbohydrate quantity is the relevant variable for most women. Whole food carbohydrates, including oats, sweet potato, brown rice, lentils, legumes, and fruit, provide the fibre, micronutrients, and slow-release energy that support hormonal function, gut health, and sustained training performance. Highly refined carbohydrates disrupt blood glucose and insulin, impair hormonal balance, and contribute to the energy crashes and cravings that undermine consistency.
Iron, calcium, and vitamin D are the three micronutrients most commonly insufficient in women's diets, with consequences ranging from chronic fatigue and poor cognitive function to bone density loss and hormonal disruption. I cover each of these in dedicated articles in this series. The short version: iron requires attention particularly in premenopausal women and those eating plant-based diets, calcium is essential for bone health across every decade, and vitamin D supplementation is appropriate for virtually every woman in the UK.
Top Tip
Build every meal around a protein source first, then add vegetables, then add complex carbohydrate. This simple structural habit, applied to every meal without exception, is the single most impactful dietary change most women can make. It stabilises blood glucose, controls appetite, supports muscle, and ensures adequate protein intake without requiring calorie counting.

Pillar Four: Hormonal Health
The hormonal system that governs the female body is one of the most sophisticated in human biology. Oestrogen, progesterone, cortisol, insulin, leptin, ghrelin, thyroid hormones, and testosterone in smaller but meaningful amounts all interact in a dynamic, continuously shifting environment. Understanding this environment is not an optional extra for women who want to optimise their health. It is fundamental.
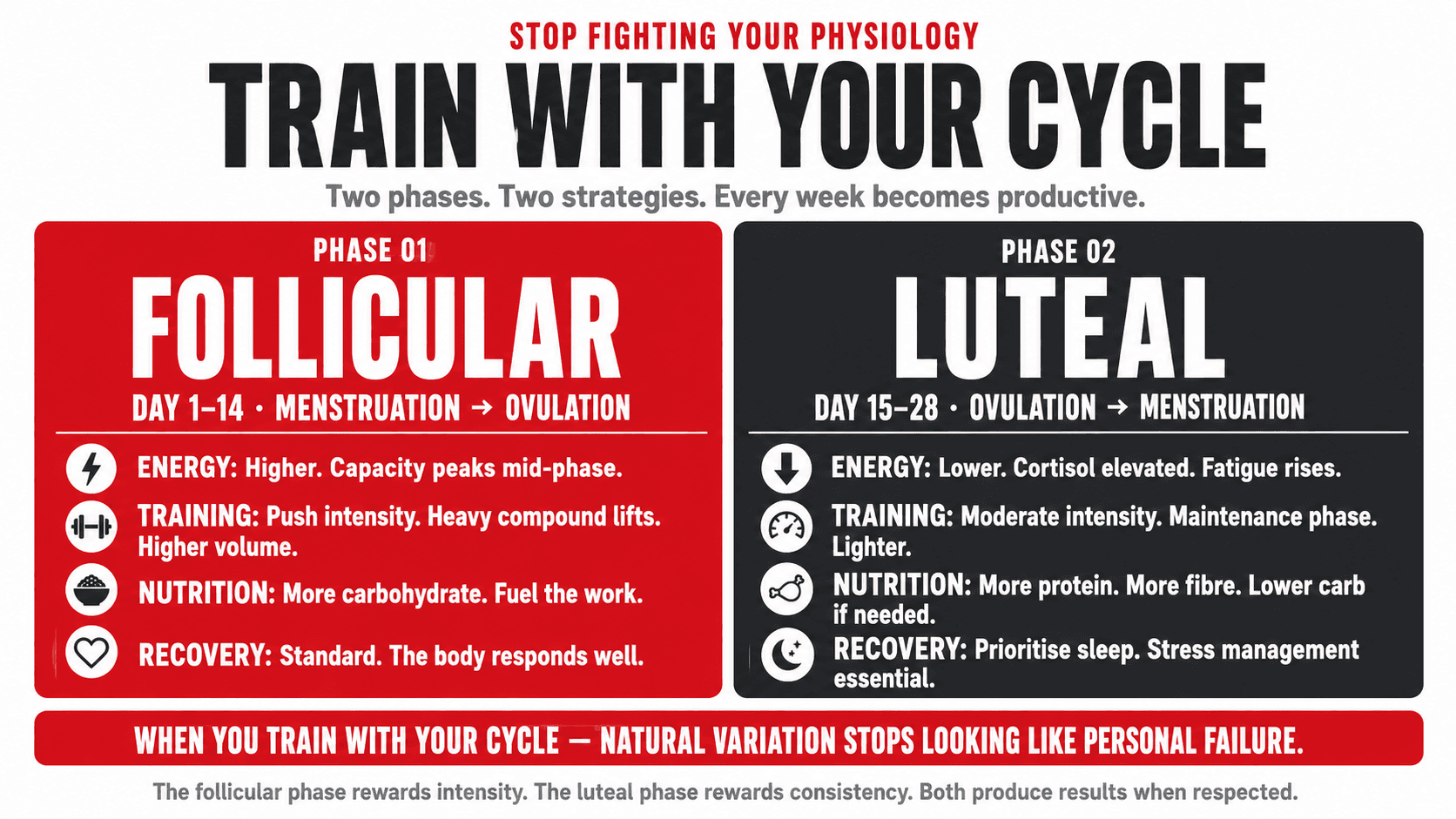
The menstrual cycle, for premenopausal women, creates a twenty-eight to thirty-five day cycle of hormonal variation that affects energy levels, strength, appetite, recovery, mood, and body composition in measurable ways. The follicular phase, from menstruation to ovulation, is typically the higher-energy, higher-strength phase when training intensity can be pushed more effectively. The luteal phase, from ovulation to menstruation, is typically characterised by higher cortisol, greater water retention, increased appetite, and a tendency toward fatigue and mood disruption. Women who understand this pattern train and eat accordingly rather than interpreting natural physiological variation as personal failure.
Cortisol and the female body deserve specific attention. Women are more susceptible to dysregulation of the hypothalamic-pituitary-adrenal axis, the stress response system that governs cortisol production, than men. Chronic stress, under-fuelling, excessive training load, poor sleep, and unresolved psychological pressure all elevate cortisol in women, with consequences that include disrupted menstrual cycles, increased visceral fat storage, impaired thyroid function, and worsened hormonal symptoms across the reproductive lifespan (6).
Managing cortisol is not about eliminating stress, which is neither possible nor desirable. It is about preventing the chronic, sustained elevation that impairs the systems described above. The practical tools are consistent: adequate sleep, appropriate training load with programmed recovery, sufficient food, and deliberate stress management practices.
Top Tip
If you are experiencing irregular periods, persistent fatigue that does not resolve with sleep, unexplained weight gain particularly around the middle, significant mood changes, or loss of libido, these are potential signals of hormonal dysregulation that warrant a conversation with your GP. Asking for a hormonal panel including oestrogen, progesterone, thyroid function, cortisol, and iron is a reasonable starting request. Do not dismiss these symptoms as normal. They are meaningful information.
Pillar Five: Recovery
Recovery is not the absence of training. It is the period during which training adaptation actually occurs. Muscle is not built in the gym. It is built in the hours and days after the gym, during sleep when growth hormone is released in its largest pulses and muscle protein synthesis peaks. Without adequate recovery, training stimulus produces diminishing returns, and eventually negative returns.
Sleep is the most important recovery tool available and the one most consistently sacrificed by the women I work with. Seven to eight hours of quality sleep per night supports testosterone and growth hormone secretion, cortisol regulation, immune function, cognitive performance, appetite regulation, and mood. The impact of chronic sleep deprivation on female hormonal health is substantial: oestrogen and progesterone secretion, thyroid function, insulin sensitivity, and cortisol regulation are all adversely affected by insufficient sleep (7). Sleep is hormonal medicine. Treating it as the negotiable variable is one of the most common and most costly mistakes women make.
Nutrition timing as part of recovery is worth noting: consuming a protein-containing meal or snack within two hours of a training session supports muscle protein synthesis during the recovery window. This applies equally to plant-based and omnivore women. A soy protein or pea protein shake, a tofu bowl, lentil soup, Greek yoghurt with seeds, or cottage cheese and fruit are all practical options depending on dietary background.
Deload weeks, periods of reduced training volume and intensity every four to six weeks, are not a sign of weakness or inconsistency. They are a planned part of a well-designed programme. The body adapts most effectively when periods of high stimulus are followed by periods of lower demand that allow full physiological recalibration.
Top Tip
Establish a consistent wake time and protect it seven days a week, including weekends. This single habit, applied consistently, does more for sleep quality and hormonal health than any supplement or intervention. The body's circadian rhythm is set primarily by wake time. Consistency here creates a hormonal environment that supports every other health goal.
What Happens When the Foundations Are Missing
Most of the health frustrations women experience in their 30s, 40s, and 50s are not mysterious or inevitable. They are predictable consequences of the same foundational gaps repeated across millions of women simultaneously.
Low muscle mass from years of cardio-dominant training and insufficient protein produces a metabolic rate that makes fat loss progressively harder with each passing year. The body has less muscle tissue to burn energy through, and less capability to handle glucose efficiently, creating an environment where weight gain requires less provocation and weight loss requires more. This is not ageing. It is the absence of resistance training and adequate protein over time.
Hormonal disruption from chronic restriction manifests as irregular cycles, persistent fatigue, hair thinning, cold intolerance, low mood, and difficulty building or maintaining muscle. The female hormonal system requires adequate nutrition to function. Oestrogen synthesis depends on dietary fat. Thyroid function depends on sufficient calorie intake. Ovarian function responds to energy availability. Restricting food for extended periods is not a neutral act. It is a signal to the female body to reduce hormonal output (8).
Poor bone density building in the 20s and 30s from insufficient calcium, vitamin D, and resistance training creates a bone density deficit that cannot be fully recovered in later decades. The osteoporosis that causes hip fractures in women in their 70s and 80s was created by the choices and circumstances of their 20s, 30s, and 40s. The time to build bone density is before it is needed, not after it is lost.
Top Tip
You cannot undo twenty years of undereating and overtraining in three months. But you can begin building the foundations today that will determine your health, strength, and vitality in the next decade and the one after. The most important thing is not the pace of the start. It is the consistency of the direction.
How I Build These Five Pillars Into Every Programme I Write
Every client I work with, regardless of age, health history, dietary background, or starting point, is assessed against all five pillars before a single training session or meal plan is designed. Where the foundations are solid, we build on them. Where they are absent or compromised, we address them first, because experience has taught me that no programme layer placed on top of a crumbling foundation produces the result the client is paying for.
The women I have coached who achieved the most significant and lasting transformations were not necessarily the ones who started from the best position. They were the ones who understood the foundations, committed to all five pillars simultaneously, and were patient enough to let the compounding work in their favour. The body is a system. Treat it like one.
This article is the entry point to a full series on women's health that covers PCOS, weight training, fat loss, perimenopause, menopause, bone health, hormonal health, iron deficiency, cardiovascular health, mental health, and pregnancy and post-pregnancy. Every article in this series is built on the five pillars laid out here. If you want support building them into your life with the precision and accountability of one-to-one coaching, I work one-to-one with women online globally. The conversation starts whenever you are ready.
