
If you live in the UK, there is a strong chance you are vitamin D deficient. That is not scaremongering. It is what the data consistently shows. National Diet and Nutrition Survey figures indicate that approximately 1 in 5 adults in the UK has serum vitamin D levels below the threshold for deficiency, and during the winter months that number climbs substantially higher (1). Some estimates suggest that up to 40 percent of the UK adult population is insufficient or deficient in vitamin D between October and March (2). And this is not a minor nutritional footnote. Vitamin D deficiency affects your bones, your muscles, your immune system, your hormonal health, your mood, your metabolic function, and your ability to recover from training. If you are trying to transform your body, lose fat, build muscle, or improve your health, and you are walking around with inadequate vitamin D levels, you are working against yourself without even knowing it.
I test or enquire about vitamin D status with almost every client I take on. It is one of the simplest and cheapest nutritional issues to fix, and the impact of fixing it is felt across almost every system in the body. This is not a trendy biohack. It is basic nutritional housekeeping that most people are neglecting.

What Vitamin D Actually Is
Vitamin D is technically not a vitamin at all. It is a secosteroid hormone precursor that your body produces when your skin is exposed to ultraviolet B (UVB) radiation from sunlight. When UVB rays hit your skin, a cholesterol derivative called 7-dehydrocholesterol is converted into vitamin D3 (cholecalciferol). This is then transported to the liver where it is converted into 25-hydroxyvitamin D (calcidiol), the form measured in blood tests, and subsequently to the kidneys where it is converted into its active hormonal form, 1,25-dihydroxyvitamin D (calcitriol) (3). The fact that vitamin D functions as a hormone rather than a simple vitamin is important because it means its influence extends far beyond the single-function role most people associate it with. It does not just help with calcium absorption. It has receptors in virtually every tissue in the body and influences the expression of over 1,000 genes (4).
Why Deficiency Is So Common in the UK
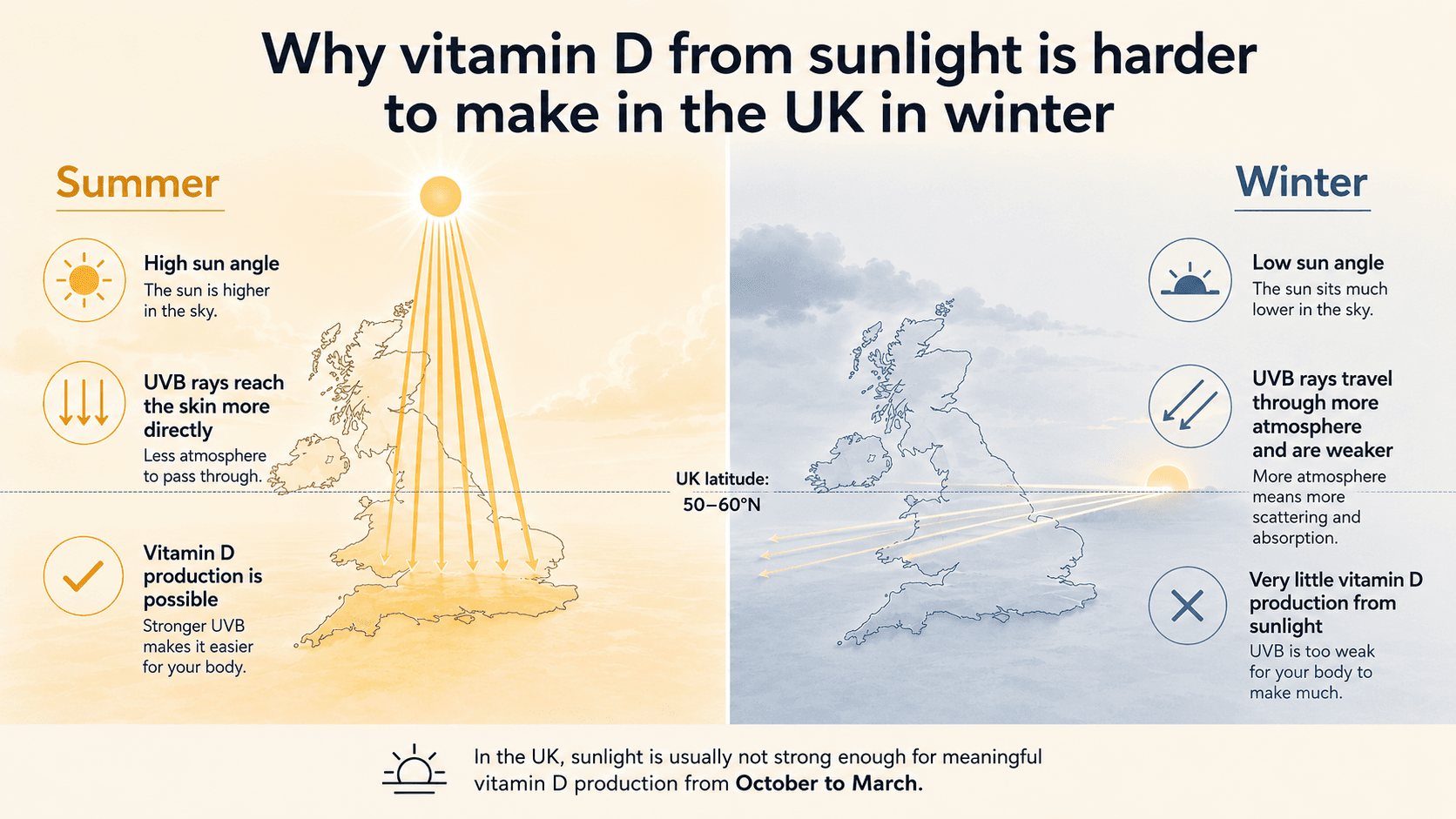
The UK sits between latitudes 50 and 60 degrees north. During the months of October through to March, the angle of the sun is too low for sufficient UVB radiation to reach the earth's surface at this latitude. This means that for roughly half the year, your body cannot produce meaningful amounts of vitamin D from sunlight regardless of how much time you spend outdoors (5). Even during the summer months, vitamin D synthesis is dependent on exposed skin, time of day (UVB is strongest between 10am and 3pm), skin pigmentation, sunscreen use, and cloud cover. People with darker skin tones require significantly more sun exposure to produce the same amount of vitamin D as those with lighter skin, because melanin acts as a natural sunscreen and reduces UVB penetration (6). This means that individuals of South Asian, African, and Caribbean heritage living in the UK are at particularly elevated risk of deficiency.
Modern lifestyles compound the problem further. Most people spend the vast majority of their day indoors. Office workers, shift workers, and anyone commuting during early morning and evening hours gets minimal sun exposure even during the summer. Add to this the limited dietary sources of vitamin D, which I will cover shortly, and you have a situation where deficiency is not the exception. It is the norm. The UK government recommends that all adults consider supplementing with vitamin D during autumn and winter, and that certain at-risk groups supplement year-round (7). This is one of the few supplements with an official public health recommendation behind it.
What Vitamin D Does in Your Body
The role most people know about is calcium metabolism and bone health. Vitamin D is essential for the absorption of calcium from the gut. Without adequate vitamin D, you can only absorb approximately 10 to 15 percent of dietary calcium, compared to 30 to 40 percent with sufficient levels (3). Chronic vitamin D deficiency leads to poor bone mineralisation, increased risk of stress fractures, and in severe cases osteomalacia in adults and rickets in children. For anyone doing resistance training, bone health is not optional. Strong bones are the scaffolding that supports strong muscles.
But the impact of vitamin D goes far beyond bones. Research has identified vitamin D receptors in skeletal muscle tissue, and studies have shown that adequate vitamin D levels are associated with improved muscle function, strength, and reduced risk of falls in older adults (8). Vitamin D plays a significant role in immune regulation. A meta-analysis published in the BMJ found that vitamin D supplementation reduced the risk of acute respiratory tract infections, with the greatest benefit seen in individuals who were deficient at baseline (9). It influences insulin sensitivity and glucose metabolism, with low levels being associated with increased risk of type 2 diabetes and metabolic syndrome (10). It affects mood and mental health, with deficiency linked to increased risk of depression and seasonal affective disorder (11). And emerging evidence connects vitamin D status to testosterone levels in men, cardiovascular health, and even cancer risk, though these areas require further research.
Vitamin D, Fat Loss, and Body Composition
For clients pursuing fat loss, there is a relationship between vitamin D status and body composition that deserves attention. Vitamin D is a fat-soluble vitamin, which means it gets sequestered in adipose tissue. Individuals with higher body fat percentages tend to have lower circulating vitamin D levels because a greater proportion is trapped in fat stores rather than being available in the bloodstream (12). This creates a cycle where carrying excess body fat increases the risk of deficiency, and deficiency may in turn make fat loss harder by impairing insulin sensitivity, increasing inflammation, and disrupting hormonal balance.
A study published in the American Journal of Clinical Nutrition found that vitamin D supplementation in overweight and obese women on a calorie-restricted diet resulted in significantly greater fat loss compared to placebo (13). This does not mean vitamin D is a fat burner. It means that correcting a deficiency removes a metabolic obstacle. When vitamin D levels are adequate, insulin functions more efficiently, inflammation is better controlled, and the hormonal environment is more favourable for fat mobilisation. For clients who are overweight, training hard, eating in a deficit, and still not seeing the fat loss they expect, vitamin D status is one of the first things I check.

Vitamin D and Training Performance
There is a direct relationship between vitamin D status and physical performance. A review published in the Journal of Science and Medicine in Sport found that athletes with adequate vitamin D levels demonstrated superior muscular strength, power output, and reduced injury rates compared to those with low levels (14). Vitamin D influences muscle fibre composition and contractile function, and deficiency has been associated with muscle weakness, fatigue, and an increased susceptibility to musculoskeletal injuries including stress fractures and muscle strains.
For my clients who train consistently, maintaining adequate vitamin D is part of the foundation that keeps them healthy, recovering well, and progressing. A deficiency does not just make you feel flat and tired. It tangibly reduces your capacity to perform and adapt. You cannot train at your best if the basic biological systems that support muscular function are compromised. Correcting a vitamin D deficiency will not turn you into a different athlete overnight, but it removes a ceiling that many people do not realise is there.
Food Sources of Vitamin D
Dietary sources of vitamin D are limited and it is very difficult to meet your requirements through food alone. The richest natural source is oily fish. Salmon, mackerel, sardines, and herring provide roughly 10 to 20 micrograms per serving depending on whether the fish is wild or farmed (wild salmon contains substantially more). Egg yolks contain small amounts, typically 1 to 2 micrograms per yolk. Liver contains vitamin D but is not commonly consumed. Some foods are fortified with vitamin D, including certain milks, cereals, orange juices, and plant-based milk alternatives such as fortified soy milk, oat milk, and almond milk. Mushrooms exposed to UV light are one of the few plant-based sources, though the form they contain (D2) is less efficiently used by the body than the D3 found in animal sources and supplements (15).
For vegetarian clients, eggs and fortified dairy products provide some vitamin D, but rarely enough to maintain optimal levels without supplementation. For vegan clients, the situation is even more challenging. Fortified plant milks, UV-exposed mushrooms, and fortified cereals contribute, but supplementation is essentially non-negotiable. The good news is that vegan-friendly vitamin D3 supplements derived from lichen are now widely available and equally effective as animal-derived D3.

How Much Vitamin D Do You Need
The UK government recommendation is 10 micrograms (400 IU) per day for all adults during autumn and winter. However, many researchers and clinicians, myself included, consider this a minimum to prevent outright deficiency rather than a dose that achieves optimal levels. The Endocrine Society recommends 1,000 to 2,000 IU per day for most adults to maintain serum 25-hydroxyvitamin D levels above 75 nmol/L (30 ng/mL), which is widely considered the threshold for sufficiency rather than just avoiding deficiency (16). For individuals who are already deficient, a higher loading dose may be appropriate under medical supervision to bring levels up before switching to a maintenance dose.
I typically recommend 1,000 to 2,000 IU of vitamin D3 per day for most of my clients as a year-round baseline. For clients with darker skin tones, higher body fat percentages, limited sun exposure, or confirmed deficiency on blood work, I may recommend 3,000 to 4,000 IU per day, always with the advice to retest after 8 to 12 weeks to confirm levels are improving. Vitamin D is fat-soluble, so it should be taken with a meal containing dietary fat to maximise absorption. The upper tolerable limit set by the European Food Safety Authority is 4,000 IU per day, and toxicity is extremely rare at doses below 10,000 IU per day (17). That said, more is not always better, and blood testing is the only way to know exactly where you stand.
Top Tips for Optimising Your Vitamin D Status
Get Your Levels Tested
This is the single most important step. A simple blood test measuring serum 25-hydroxyvitamin D will tell you exactly where you are. Ask your GP or order a home test kit. Aiming for a level of 75 to 125 nmol/L puts you in the optimal range. You cannot manage what you do not measure, and guessing your vitamin D status is not good enough when testing is so accessible and affordable.
Supplement Year-Round if You Live in the UK
The October to March sun gap means you are depleting stores for half the year without replenishment. Even during summer, inconsistent sun exposure, indoor lifestyles, and sunscreen use mean most people are not producing enough. A daily supplement of 1,000 to 2,000 IU removes the guesswork and provides a reliable baseline regardless of the season or your schedule.
Choose Vitamin D3 Over D2
Vitamin D3 (cholecalciferol) is more effective at raising and maintaining serum vitamin D levels than D2 (ergocalciferol) (15). Most quality supplements use D3. Vegan clients should look for D3 derived from lichen, which is now widely available and equally bioavailable as animal-sourced D3.

Take It With Fat
Vitamin D is a fat-soluble vitamin. Taking it alongside a meal containing dietary fat, whether that is eggs and avocado at breakfast, a handful of nuts, or any meal with olive oil or butter, significantly improves absorption. Taking it on an empty stomach or with a fat-free meal reduces how much your body actually takes up.
Pair It With Vitamin K2
Vitamin K2 works synergistically with vitamin D to direct calcium into bones and teeth rather than allowing it to accumulate in soft tissues and arteries. A combined vitamin D3 and K2 supplement is a practical choice that supports both bone health and cardiovascular health (18). Many quality vitamin D supplements now include K2 as standard.
Get Sensible Sun Exposure When You Can
During the summer months, aim for 10 to 20 minutes of direct sun exposure on your forearms, hands, and lower legs between 10am and 3pm, several times per week, without sunscreen. This is enough to stimulate meaningful vitamin D production without significantly increasing skin cancer risk. After that initial exposure, apply sunscreen as normal. This is not a replacement for supplementation, but it complements it and supports your overall levels.
Be Aware of Your Individual Risk Factors
If you have darker skin, a higher body fat percentage, spend most of your day indoors, cover your skin for cultural or religious reasons, are over 65 (skin synthesis declines with age), or follow a strict vegan diet without fortification, your risk of deficiency is elevated. These individuals often need the higher end of the supplementation range and should prioritise blood testing to confirm adequacy.
The Bottom Line
Vitamin D deficiency is one of the most common and most easily correctable nutritional issues in the UK. It affects your bones, your muscles, your immune system, your mood, your metabolic health, your body composition, and your training performance. If you have never had your levels tested, get tested. If you are not supplementing, start. A daily dose of 1,000 to 2,000 IU of vitamin D3, taken with food, year-round, is one of the simplest and most impactful things you can do for your health. It costs pennies per day and the evidence supporting it is rock solid.
If you want a personalised nutrition, training, and supplementation plan that accounts for your individual needs, your health status, your goals, and your dietary preferences, get in touch through trperformancecoaching.com. I work one-to-one with clients online globally, across every dietary background. Whether you eat meat, are vegetarian, vegan, or somewhere in between, I will build something that works for your body and your life.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- Public Health England. National Diet and Nutrition Survey: Results from Years 9 to 11 (2016/2017 to 2018/2019). PHE publications gateway number: GOV-9740. 2020.
- Sheridan C. Vitamin D deficiency in the UK population: a growing epidemic. British Journal of General Practice. 2019; 69(680): 142-143.
- Holick MF. Vitamin D deficiency. New England Journal of Medicine. 2007; 357(3): 266-281.
- Hossein-nezhad A, Holick MF. Vitamin D for health: a global perspective. Mayo Clinic Proceedings. 2013; 88(7): 720-755.
- Webb AR, Kline L, Holick MF. Influence of season and latitude on the cutaneous synthesis of vitamin D3: exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. Journal of Clinical Endocrinology and Metabolism. 1988; 67(2): 373-378.
- Clemens TL, Adams JS, Henderson SL, Holick MF. Increased skin pigment reduces the capacity of skin to synthesise vitamin D3. The Lancet. 1982; 319(8263): 74-76.
- Scientific Advisory Committee on Nutrition. Vitamin D and Health. London: The Stationery Office; 2016.
- Tomlinson PB, Joseph C, Angioi M. Effects of vitamin D supplementation on upper and lower body muscle strength levels in healthy individuals: a systematic review with meta-analysis. Journal of Science and Medicine in Sport. 2015; 18(5): 575-580.
- Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017; 356: i6583.
- Pittas AG, Lau J, Hu FB, Dawson-Hughes B. The role of vitamin D and calcium in type 2 diabetes: a systematic review and meta-analysis. Journal of Clinical Endocrinology and Metabolism. 2007; 92(6): 2017-2029.
- Anglin RE, Samaan Z, Walter SD, McDonald SD. Vitamin D deficiency and depression in adults: systematic review and meta-analysis. British Journal of Psychiatry. 2013; 202(2): 100-107.
- Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. American Journal of Clinical Nutrition. 2000; 72(3): 690-693.
- Mason C, Xiao L, Imayama I, et al. Vitamin D3 supplementation during weight loss: a double-blind randomized controlled trial. American Journal of Clinical Nutrition. 2014; 99(5): 1015-1025.
- Farrokhyar F, Tabasinejad R, Dao D, et al. Prevalence of vitamin D inadequacy in athletes: a systematic review and meta-analysis. Sports Medicine. 2015; 45(3): 365-378.
- Tripkovic L, Lambert H, Hart K, et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. American Journal of Clinical Nutrition. 2012; 95(6): 1357-1364.
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology and Metabolism. 2011; 96(7): 1911-1930.
- European Food Safety Authority. Scientific opinion on the tolerable upper intake level of vitamin D. EFSA Journal. 2012; 10(7): 2813.
- van Ballegooijen AJ, Pilz S, Tomaschitz A, Grubler MR, Verheyen N. The synergistic interplay between vitamins D and K for bone and cardiovascular health: a narrative review. International Journal of Endocrinology. 2017; 2017: 7454376.
