If you have ever typed best diet for fat loss into a search engine, you will have been met with a wall of contradictory advice. One article tells you keto is the answer. The next tells you keto will destroy your health. Someone swears by intermittent fasting. Someone else says it wrecks your hormones. Low fat worked in the 1990s. Low carb works now. The Mediterranean diet wins every award. The carnivore diet has a cult following. Every dietary camp has passionate advocates, cherry-picked studies, and transformation photos that seem to prove their case. And every person standing in the supermarket trying to figure out what to put in their trolley ends up more confused than when they started.
I have worked with meat eaters, vegetarians, vegans, and people who fall somewhere in between. I have coached executives who eat out five nights a week and parents who batch-cook everything on a Sunday. I have worked with clients managing type 2 diabetes, PCOS, insulin resistance, hypertension, and a dozen other conditions that demand specific nutritional considerations. And after all of those years and all of those clients, I can tell you with absolute confidence: there is no single best diet for fat loss. There never has been. The research proves it, my coaching experience confirms it, and the sooner you stop looking for the perfect diet and start finding the right approach for you, the sooner you will get results.
The Search for the Perfect Diet Is Keeping You Stuck
The diet industry is worth billions precisely because it convinces people that the next programme, the next protocol, the next macronutrient ratio is the one that will finally work. Every year brings a new trend. Every trend comes with a book, a podcast, a supplement line, and a social media personality telling you this is the answer. And every time, people abandon what they were doing, jump to the new approach, follow it rigidly for three weeks, find it unsustainable, quit, and go searching for the next one.
This is what I call diet-hopping, and it is one of the most destructive patterns I see in people who struggle with fat loss. They have tried everything and succeeded at nothing, not because they lack discipline but because they keep chasing the mythical perfect diet instead of committing to any imperfect but consistent approach. The irony is that almost any structured dietary approach will produce fat loss if it creates a calorie deficit and is followed consistently. The problem was never the diet. The problem was always the match between the diet and the person.
What the Research Actually Says About Diet Comparisons
The scientific literature on this question is remarkably consistent, and the answer is not what the diet industry wants you to hear. A landmark network meta-analysis published in the BMJ in 2020 compared 14 popular named dietary programmes, including low carbohydrate, low fat, Mediterranean, Atkins, DASH, Zone, Ornish, Jenny Craig, and others, across 121 randomised controlled trials involving nearly 22,000 adults. The results were striking: at six months, most diets produced modest weight loss compared to usual eating. By twelve months, the differences between diets had largely disappeared (1). The diet that produced the best results was whichever one the individual actually followed.
A separate meta-analysis published in JAMA analysed 48 randomised trials comparing named diet programmes and found that any dietary approach, whether low carbohydrate or low fat, produced clinically meaningful weight loss provided it was adhered to. The differences between individual diets were small and clinically insignificant compared to the difference between following a diet and not following one at all (2). An earlier JAMA study comparing Atkins, Ornish, Weight Watchers, and Zone diets found that weight loss at 12 months was similar across all four approaches, and adherence was the strongest predictor of success regardless of which diet was assigned (3).
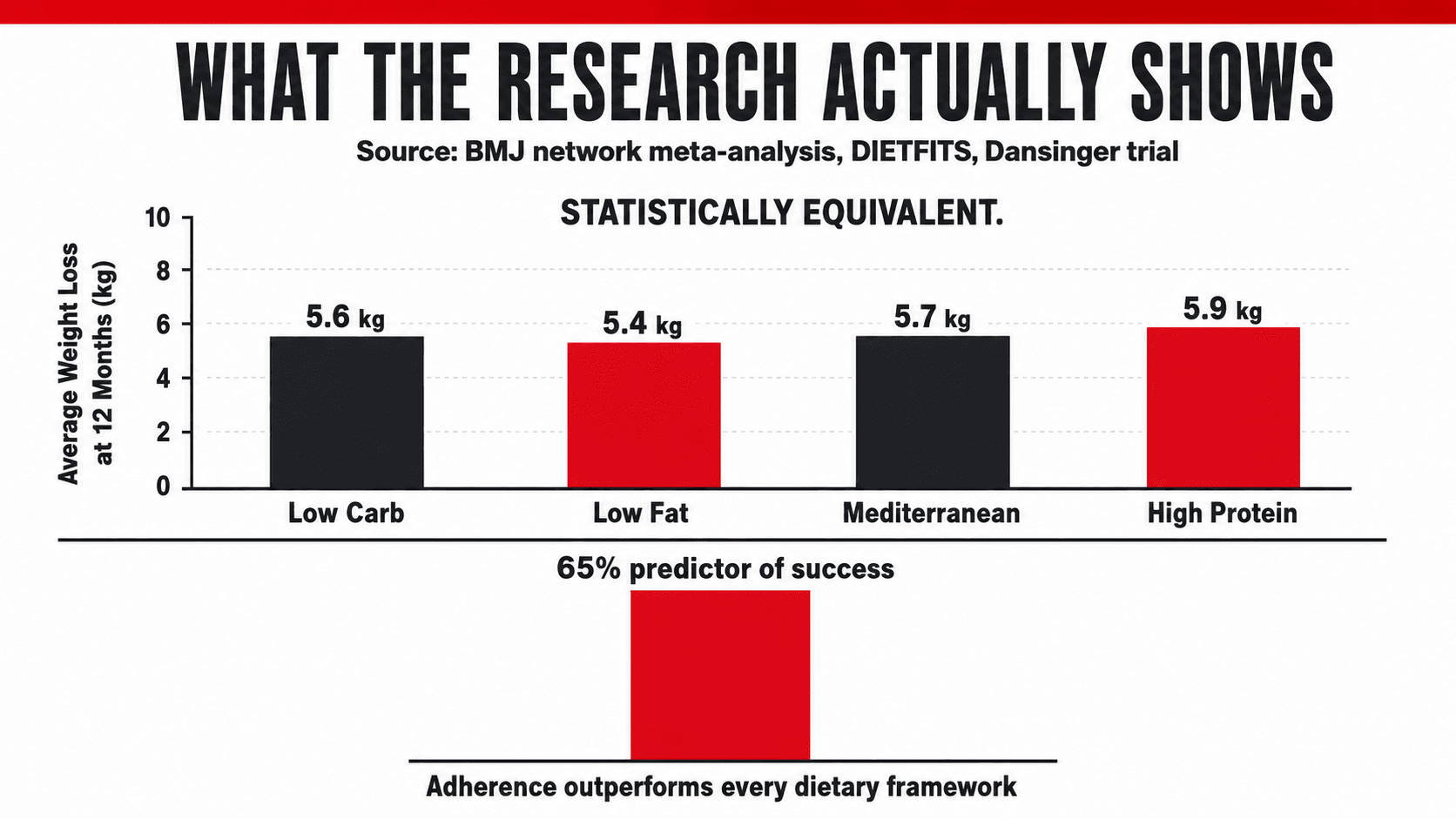
The DIETFITS trial, one of the most rigorously controlled weight loss studies ever conducted, randomised over 600 participants to either a healthy low-fat or a healthy low-carbohydrate diet for 12 months. Both groups received extensive behavioural support. The result? No significant difference in weight loss between the two groups. Both lost an average of 5 to 6 kilograms. There was no interaction between genotype pattern and diet, and no interaction between baseline insulin secretion and diet (4). The researchers concluded that the specific macronutrient composition mattered far less than the overall quality of the diet and the individual's ability to sustain it.
The message from decades of controlled research is unequivocal: the best diet for fat loss is the one you can follow consistently, that puts you in a calorie deficit, that provides adequate protein, and that you can maintain for long enough to produce and sustain meaningful results.
Popular Diets Compared: An Honest Assessment
The following table provides an honest, evidence-based overview of the most popular dietary approaches for fat loss. I have included their core principles, what the evidence says about their effectiveness, who they tend to work best for, and their key limitations. No diet scores a perfect mark across every category, because no perfect diet exists.
| Diet | Core Principle | Evidence for Fat Loss | Best Suited To | Key Limitations | Vegetarian / Vegan Friendly |
|---|---|---|---|---|---|
| Low Carbohydrate | Reduce carbs to 50-130g per day. Increase protein and fat. | Effective short-term. Slight edge at 6 months. No advantage at 12+ months when calories matched (1, 2). | Insulin-resistant clients. People who overeat carbs. Those who prefer higher fat foods. | Can limit training performance. Restrictive long-term. Adherence declines after 3-6 months. | Possible but harder for vegans. Requires careful planning. |
| Ketogenic | Very low carb (<50g/day). High fat. Moderate protein. Induces ketosis. | Rapid initial weight loss (mostly water). Appetite suppression. No long-term advantage over balanced diets (5). | Short-term kickstart. People who respond well to rigid rules. Some epilepsy patients. | Very restrictive. Eliminates many nutrient-dense foods. Poor long-term adherence. Impractical for most vegetarians/vegans. | Very difficult for vegetarians. Practically impossible for vegans. |
| Low Fat | Reduce dietary fat to <30% of calories. Higher carb, moderate protein. | Effective when calorie deficit achieved. No significant difference from low carb at 12 months (4). | People who prefer carb-rich foods. Clients comfortable with volume eating from grains and legumes. | Can leave some people hungry due to lower satiety of refined carbs. Fat restriction may affect hormone production if too extreme. | Very compatible. Naturally aligns with many plant-based diets. |
| Mediterranean | Emphasises olive oil, fish, vegetables, legumes, whole grains, moderate wine. | Strong evidence for cardiovascular health. Comparable weight loss to other approaches when calorie-controlled (1). | People who enjoy cooking. Those prioritising heart health. Sustainable long-term approach. | Not inherently a fat loss diet. Requires calorie awareness to avoid surplus. Higher fat foods can be calorically dense. | Adaptable. Replace fish with legumes, tofu, tempeh for vegetarian/vegan versions. |
| Intermittent Fasting (16:8) | Restrict eating to an 8-hour window. Fast for 16 hours daily. | Produces similar weight loss to continuous restriction when calories are matched. No metabolic magic (6). | People who prefer fewer, larger meals. Those who naturally skip breakfast. Busy professionals. | Does not guarantee a calorie deficit. Can promote overeating in the eating window. Social limitations. May not suit those with disordered eating history. | Fully compatible with any dietary preference. |
| Flexible Dieting / IIFYM | Track macros. Eat any foods provided targets are met. | Effective when targets are hit consistently. Matches evidence on energy balance and protein adequacy. | People who want dietary freedom. Experienced dieters. Those who enjoy data and tracking. | Requires consistent tracking. Can normalise poor food quality. Does not address food quality or micronutrients adequately. | Fully compatible. |
| High Protein | Protein set at 1.6-2.2g/kg. Remaining calories from carbs and fats. | Strong evidence for muscle preservation, satiety, and improved body composition during fat loss (7, 8). | Almost everyone in a fat loss phase. Especially those who train. My default starting point. | Requires planning. Can be expensive. Vegetarians and vegans need protein-dense sources. | Compatible with all dietary backgrounds using tofu, tempeh, seitan, soy/pea protein, legumes, dairy alternatives. |
Five Questions That Will Help You Find the Right Diet for You
Rather than asking which diet is best, ask yourself these five questions. Your answers will point you towards the approach that is most likely to produce sustainable results for your body, your preferences, and your life.
Question One: What Can I Actually Sustain for Six Months or More? This is the single most important question and it should be answered first. If you cannot see yourself following an approach for at least six months, it is the wrong approach regardless of how effective it looks on paper. A moderate calorie deficit with foods you enjoy, prepared in ways that fit your lifestyle, will always outperform a theoretically optimal diet that you abandon after three weeks. Adherence is not a weakness to be overcome. It is the primary determinant of success (1, 2, 3).
Question Two: Does This Approach Give Me Enough Protein? Regardless of which dietary framework you choose, protein must be prioritised. The evidence for higher protein intakes during fat loss is overwhelming: it preserves lean muscle mass, increases satiety, has the highest thermic effect of any macronutrient, and produces better body composition outcomes (7, 8). I set protein at 1.6 to 2.2 grams per kilogram of bodyweight for virtually every fat loss client I work with. If your chosen diet cannot deliver adequate protein, it needs to be modified or replaced. For omnivores this means chicken, fish, lean meat, eggs, and dairy. For vegetarians: eggs, Greek yoghurt, cottage cheese, tofu, tempeh, paneer, and whey protein. For vegans: tofu, tempeh, seitan, edamame, soy or pea protein, lentils, and chickpeas.
Question Three: Does It Put Me in a Calorie Deficit Without Making Me Miserable? Fat loss requires a sustained calorie deficit. That is non-negotiable physics. But the deficit does not need to be extreme. A moderate deficit of 400 to 600 calories per day produces steady fat loss of approximately 0.5 to 1 kilogram per week while preserving muscle, maintaining energy, and keeping hunger manageable. If your approach leaves you constantly hungry, exhausted, and unable to think about anything other than food, the deficit is too aggressive or the food choices are wrong. A good fat loss diet should feel like a slight stretch, not a war of attrition.
Question Four: Does It Fit My Medical and Metabolic Needs? This is where individualisation becomes critical and where a one-size-fits-all approach breaks down. If you have insulin resistance or type 2 diabetes, managing carbohydrate type and timing becomes more important. If you have PCOS, prioritising lower glycemic carbohydrate sources and adequate protein supports hormonal balance. If you have high blood pressure, sodium awareness and a diet rich in potassium, magnesium, and calcium (the DASH principles) is relevant. If you have coeliac disease, a gluten-free approach is non-negotiable. If you are post-menopausal, protein and calcium requirements are higher. The best diet for you is the one that accounts for your specific health profile, not just your weight loss goal.
Question Five: Does It Align With My Values and Preferences? I am a lifelong vegetarian. I understand what it is like to be told that the best diet for results involves foods you do not eat. The truth is that fat loss works equally well on a plant-based diet, a mixed diet, or any other pattern that meets the fundamental requirements of a calorie deficit, adequate protein, and sufficient micronutrient intake. Your ethical beliefs, your cultural food traditions, your family's eating patterns, and your personal enjoyment of food all matter. A diet that conflicts with your values will not last. A diet that works with them will.

Why Adherence Matters More Than Any Macronutrient Ratio
The Dansinger trial, published in JAMA, randomised 160 participants to Atkins (low carb), Ornish (very low fat), Weight Watchers (calorie counting), or Zone (balanced macros) and followed them for 12 months. The dietary adherence rate predicted weight loss far more strongly than the diet itself. Participants with the highest adherence scores lost the most weight regardless of which group they were assigned to, and participants with the lowest adherence lost the least regardless of which theoretically superior diet they were following (3). The study demonstrated what every experienced coach already knows: consistency beats optimality. Every single time.
A systematic review of weight maintenance studies found that only around 25 percent of people who lose weight through dieting maintain their results long term (9). The factors that predicted successful maintenance were not the specific diet used but rather continued contact with a health professional, structured behavioural support, regular self-monitoring, and a flexible rather than rigid approach to eating. In other words, the process of coaching and accountability matters more than the macronutrient prescription.
This is why I never prescribe a single dietary template to every client. Some of my clients thrive on a higher carbohydrate, lower fat approach because they train hard and love rice, oats, and fruit. Others prefer a lower carbohydrate, higher fat approach because it keeps their appetite controlled and they enjoy eggs, cheese, nuts, and avocado. Some eat three structured meals a day. Others prefer two larger meals with a smaller snack. Some fast until noon. Others need breakfast to function. The macronutrient split is a variable. The calorie deficit and protein target are the constants. And the coaching, the accountability, and the ongoing adjustment are what make the difference between a temporary result and a permanent one.
Top Tips: Finding Your Right Dietary Approach
Stop looking for the best diet and start looking for your diet. The research is unambiguous: no single dietary approach is meaningfully superior for fat loss when calories and protein are equated. The best approach is the one that fits your life, your preferences, and your medical needs, and that you can follow consistently for months and years.
Start with protein. Before you choose any dietary framework, make sure it can deliver 1.6 to 2.2 grams of protein per kilogram of bodyweight per day. This is the single non-negotiable macronutrient target for anyone pursuing fat loss. Build every meal around a protein source first, then add everything else.
Think in terms of traffic lights, not forbidden foods. Green light foods are whole, minimally processed, nutrient-dense foods that make up 80 percent or more of your intake. Amber light foods are those you eat in moderation and with awareness. Red light foods are those you know trigger overeating or derail your plan. This framework works with any dietary approach and avoids the all-or-nothing mentality that destroys adherence.

Give any new approach at least four to six weeks before judging it. The first two weeks of any dietary change involve adaptation, water fluctuations, and psychological adjustment. You cannot judge the effectiveness of an approach until you have followed it consistently for at least a month. If you are changing diets every two weeks, you are not evaluating anything. You are just diet-hopping.
Prioritise food quality regardless of which framework you choose. Whole, minimally processed foods are more satiating, more nutrient-dense, and harder to overeat than ultra-processed alternatives. This applies whether you eat low carb, low fat, Mediterranean, plant-based, or any other pattern. The quality of your food determines the quality of your results.
Do not let perfection delay progress. You do not need the optimal macronutrient ratio, the ideal meal timing, or the perfect supplement stack to start losing fat. You need a moderate calorie deficit, adequate protein, resistance training, and consistency. Start with those four things and refine from there. An 80 percent plan executed consistently will always outperform a 100 percent plan followed for three days.
Get professional support. The evidence consistently shows that people who work with a coach, a dietitian, or a structured programme achieve better and longer-lasting results than those who go it alone (9). This is not because you are incapable. It is because accountability, personalisation, and ongoing adjustment are the factors that separate a temporary diet from a permanent transformation.
The Bottom Line
There is no best diet for fat loss. There is only the best diet for you. The evidence from every major meta-analysis and head-to-head comparison of the past two decades confirms that the specific dietary approach matters far less than whether you can follow it consistently, whether it provides adequate protein, whether it creates a sustainable calorie deficit, and whether it accounts for your individual needs and preferences. Low carb works if you follow it. Low fat works if you follow it. Mediterranean works if you follow it. Plant-based works if you follow it. The common denominator is not the macronutrient ratio. It is the person.
If you are tired of diet-hopping and ready for an approach that is built around your body, your preferences, your medical history, and your life, get in touch. I work one-to-one with clients online globally. Whether you eat meat, are vegetarian, vegan, or anywhere in between, I will find the dietary approach that fits you and coach you through it with the structure, personalisation, and accountability that actually produces lasting results. No ideology. No dogma. Just the right plan for you.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- Ge L, Sadeghirad B, Ball GDC, et al. Comparison of dietary macronutrient patterns of 14 popular named dietary programmes for weight and cardiovascular risk factor reduction in adults: systematic review and network meta-analysis of randomised trials. BMJ. 2020; 369: m696.
- Johnston BC, Kanters S, Bandayrel K, et al. Comparison of weight loss among named diet programs in overweight and obese adults: a meta-analysis. JAMA. 2014; 312(9): 923-933.
- Dansinger ML, Gleason JA, Griffith JL, Selker HP, Schaefer EJ. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: a randomized trial. JAMA. 2005; 293(1): 43-53.
- Gardner CD, Trepanowski JF, Del Gobbo LC, et al. Effect of low-fat vs low-carbohydrate diet on 12-month weight loss in overweight adults and the association with genotype pattern or insulin secretion: the DIETFITS randomized clinical trial. JAMA. 2018; 319(7): 667-679.
- Bueno NB, de Melo IS, de Oliveira SL, da Rocha Ataide T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. British Journal of Nutrition. 2013; 110(7): 1178-1187.
- Cioffi I, Evangelista A, Ponzo V, et al. Intermittent versus continuous energy restriction on weight loss and cardiometabolic outcomes: a systematic review and meta-analysis of randomized controlled trials. Journal of Translational Medicine. 2018; 16(1): 371.
- Leidy HJ, Clifton PM, Astrup A, et al. The role of protein in weight loss and maintenance. American Journal of Clinical Nutrition. 2015; 101(6): 1320S-1329S.
- Morton RW, Murphy KT, McKellar SR, et al. A systematic review, meta-analysis and meta-regression of the effect of protein supplementation on resistance training-induced gains in muscle mass and strength in healthy adults. British Journal of Sports Medicine. 2018; 52(6): 376-384.
- Montesi L, El Ghoch M, Brodosi L, Calugi S, Marchesini G, Dalle Grave R. Long-term weight loss maintenance for obesity: a multidisciplinary approach. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy. 2016; 9: 37-46.