The Most Limiting Belief in Health and Fitness Has No Scientific Basis
Neuroplasticity and health behaviour change sit at the intersection of two fields that, when their findings are combined, demolish the single most damaging and most widespread belief in health coaching: the belief that the adult brain is fixed, that habits formed over decades cannot be meaningfully changed, that the person is too old, too ingrained, or too fundamentally wired to build the neural architecture of a different relationship with their body, their food, and their health.
The scientific consensus on adult neuroplasticity, established primarily through the work of Michael Merzenich at the University of California San Francisco and popularised through Norman Doidge's landmark work The Brain That Changes Itself, is unambiguous: the adult brain retains a substantial capacity for structural reorganisation in response to experience, learning, and repeated behaviour throughout the entire lifespan. This is not a marginal or contested finding. It is one of the most thoroughly replicated and most practically significant discoveries in neuroscience of the past fifty years. The brain that the person with a thirty-year sedentary habit inhabits is not a fixed structure whose patterns are permanent. It is a dynamic, experience-dependent system whose architecture reflects its history and can be changed by changing that history. (1)
The implications for anyone who has been told, or who has told themselves, that they are too old to build new habits, too set in their ways to change their relationship with food, too wired for sedentary behaviour to sustain a training programme, are direct and liberating. The belief is not an accurate description of the biology. It is a belief with no scientific basis, held with the authority of long personal experience, and functioning as precisely the kind of ceiling that prevents real change. It is not the brain that cannot change. It is the belief about the brain.
“The brain is the most complex thing we have yet discovered in our universe.”
— James Watson
What Neuroplasticity Actually Is: The Science Behind the Brain That Changes
Neuroplasticity refers to the brain's capacity to reorganise its structure, function, and connections in response to experience, learning, injury, or environmental change. It operates at multiple levels simultaneously, from the synaptic level (the strengthening or weakening of connections between individual neurons based on their pattern of activation) to the cortical level (the reorganisation of the functional geography of the brain's surface in response to sustained changes in sensory or motor experience) to the structural level (the physical growth of new neurons in specific regions and the formation of entirely new neural circuits in response to learning and practice). (2)
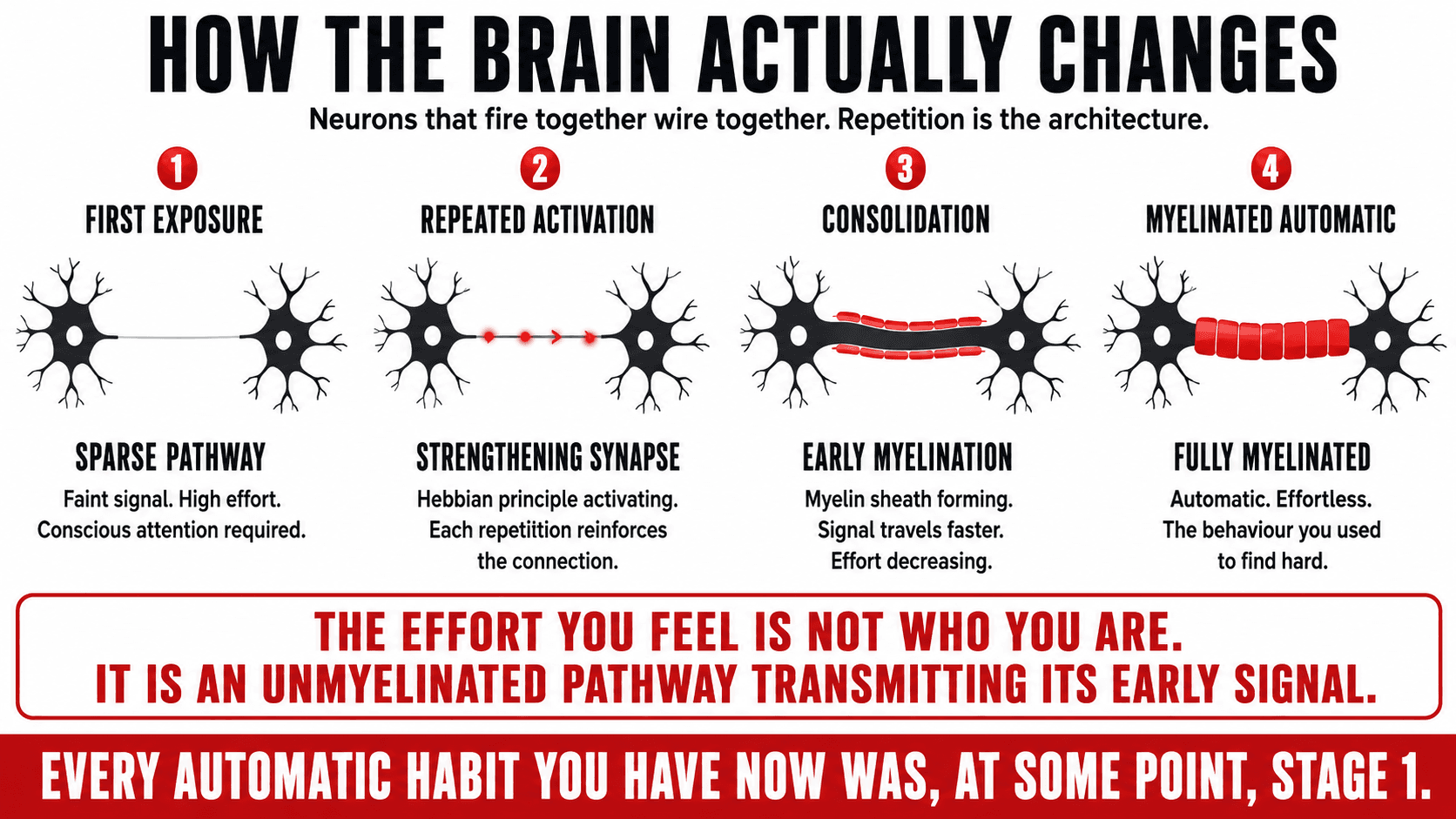
The Hebbian principle, often summarised as neurons that fire together wire together, provides the fundamental mechanism of neuroplasticity. When two neurons are consistently activated in close temporal proximity, the synaptic connection between them is strengthened. The more frequently the pattern of activation is repeated, the more the connection is reinforced, and the more efficiently the signal travels between the neurons. This is the biological basis for habit formation: every time a behaviour is executed, the neural circuit that underlies it is marginally strengthened. Every time a behaviour is not executed, the circuit is marginally weakened through a complementary process. Over time, frequent repetition produces a well-established, efficiently conducting neural pathway. Infrequent repetition produces a sparse, inefficient one. (3)
Myelination is the mechanism through which well-practiced skills become faster, more precise, and more automatic. Myelin is a fatty sheath that wraps around the axons of neurons that are frequently activated, dramatically increasing the speed and efficiency of signal transmission along those pathways. The myelinated pathway is the neurological equivalent of a high-speed data cable: it transmits information faster, more reliably, and with less energy cost than the unmyelinated alternatives. The behaviours that feel automatic, effortless, and second nature are the behaviours whose neural pathways are most thoroughly myelinated. The behaviours that feel effortful, uncertain, and demanding are the ones whose pathways are not yet myelinated, and the most direct route to making them feel automatic is the same route that produced the effortless ones: deliberate, consistent repetition over sufficient time. (4)
Key Insight: The effort you feel when executing a new health habit is not the effort of a person who is not suited to the habit. It is the effort of an unmyelinated neural pathway transmitting a signal for the early iterations of a practice that, with sufficient repetition, will become as automatic as the habits it is replacing. The effort is temporary. The pathway it is building is permanent. This is what the neuroscience actually says about why new health habits are hard at the beginning and why that difficulty is not evidence that they will remain hard.
The Neural Pathway Timeline: What Happens Inside the Brain From Week One to Week Twenty-Four
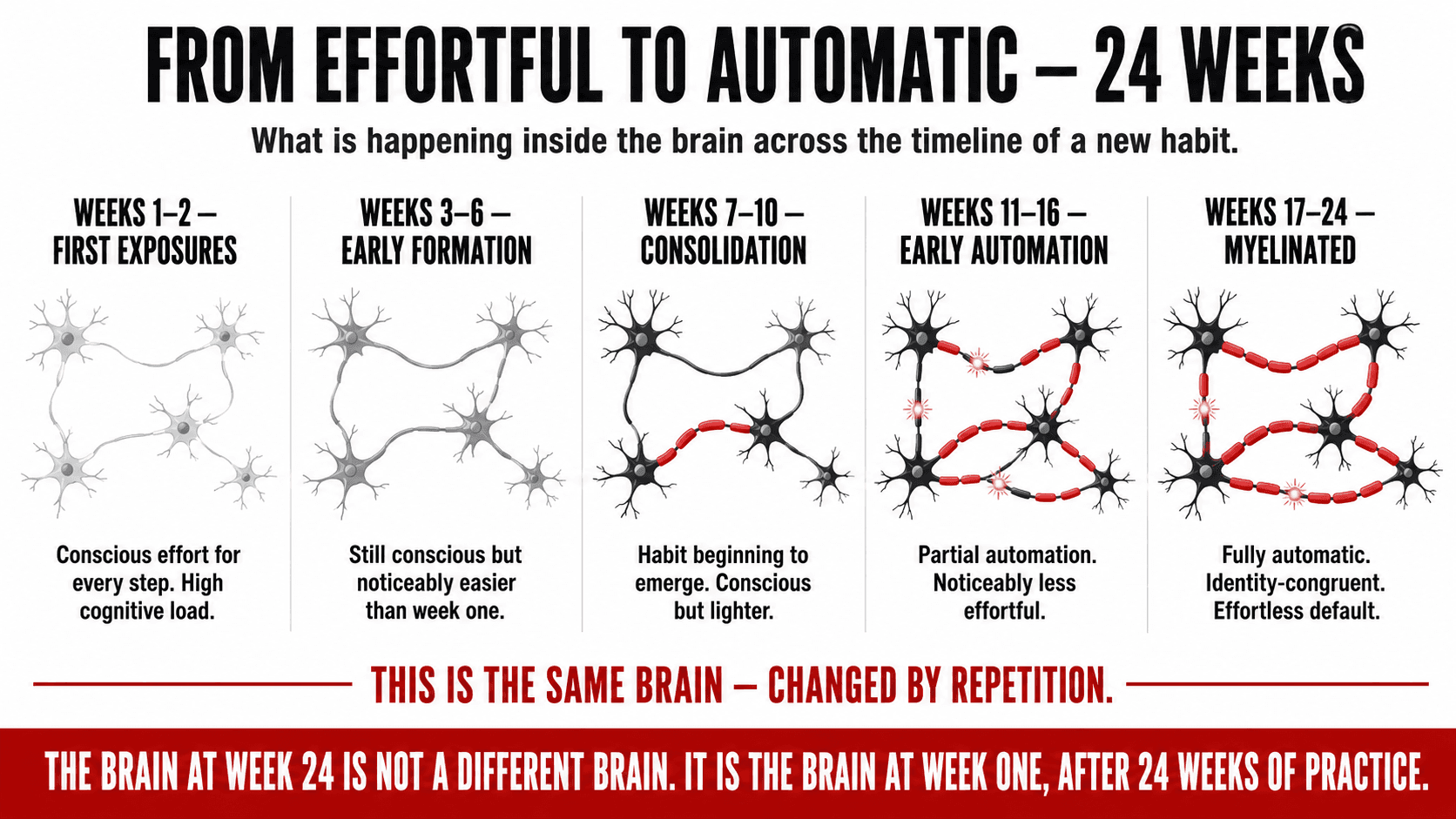
The neural pathway diagram below visualises the progression from a new, unmyelinated, effortful pathway in week one through the progressive myelination and consolidation that transforms it into the automatic, efficient, identity-congruent pattern of the established habit at week twenty-four. The progression is gradual and invisible from the outside. From the inside, it is experienced as the slow, nonlinear journey from effortful conscious execution to automatic unconscious habit that every new behaviour follows.
The Neural Pathway Timeline — From New and Effortful to Myelinated and Automatic
| Phase | Pathway 1 — Weak Signal | Pathway 2 — Forming | Pathway 3 — Strengthening | Pathway 4 — Consolidating | Pathway 5 — Myelinated |
|---|---|---|---|---|---|
| Weeks 1–2 First exposures | Faint. High effort. Conscious attention required for every step. | Not yet active | Not yet active | Not yet active | Not yet active |
| Weeks 3–6 Early formation | Strengthening. Still conscious but noticeably easier than week one. | Beginning to form. First repetitions registered. | Not yet active | Not yet active | Not yet |
| Weeks 7–10 Consolidation | Well established. Conscious but lighter. Habit beginning to emerge. | Strengthening fast. Requires attention but less cognitive load. | Forming. Early signal present. | Just beginning | Not yet |
| Weeks 11–16 Early automation | Early myelination. Partial automation. Noticeably less effortful. | Strong and reliable. Skipping feels strange now. | Established. Still conscious but efficient. | Strengthening | Early stage |
| Weeks 17–24 Myelinated | FULLY MYELINATED. Automatic. Identity-congruent. Effortless default. | Deeply embedded. Well myelinated. Runs without conscious input. | Strong and largely automatic. Feels natural. | Well established. | Consolidated. |
Every established habit began as column one, week one: faint, effortful, and requiring conscious attention for every step. The myelinated automatic response visible in weeks 17–24 is the product of weeks 1–16, not a different person's brain. It is the same brain, changed by repetition.
The Fixed Mindset vs Growth Mindset: Carol Dweck's Research Applied to Health
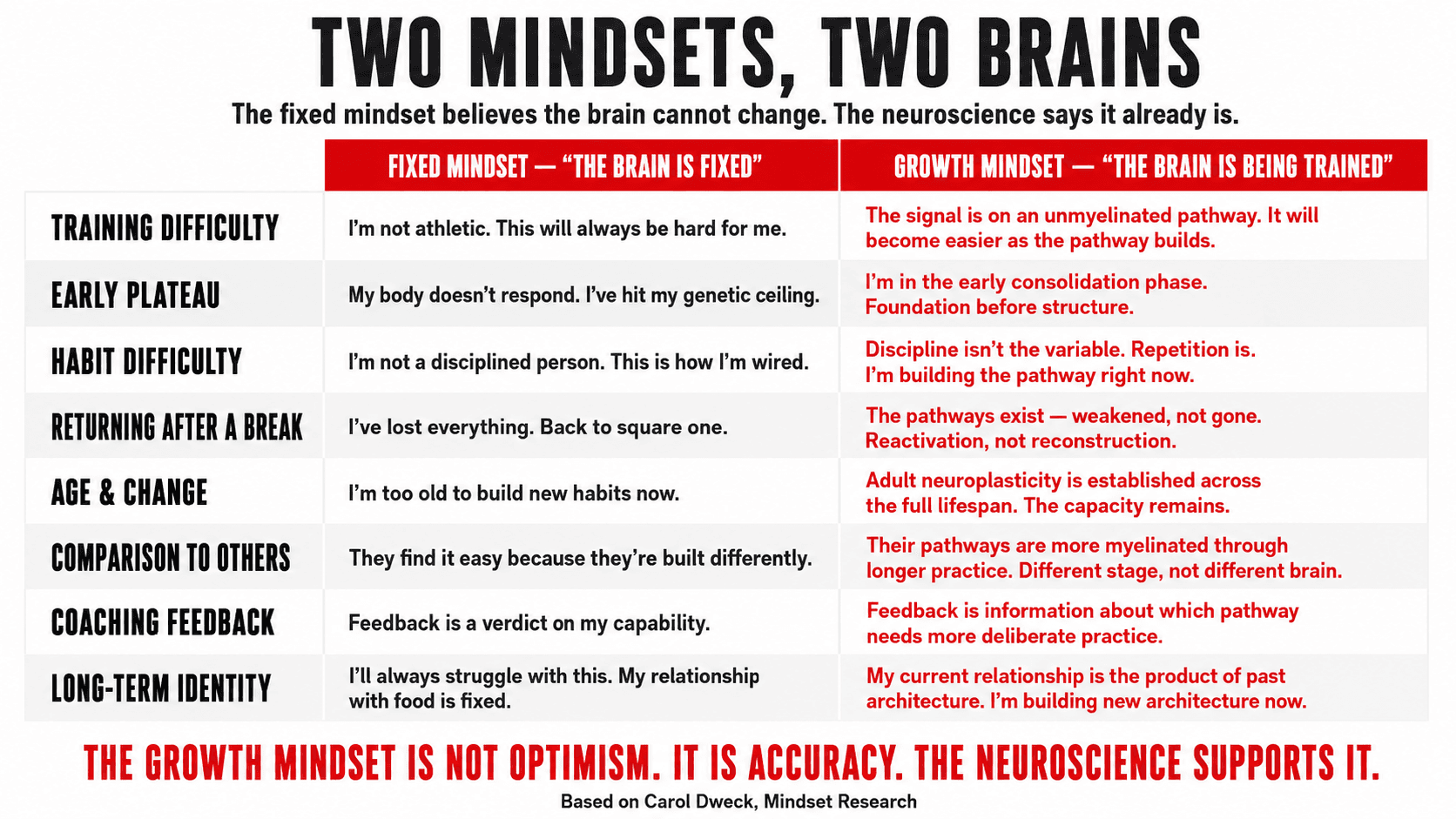
Carol Dweck's decades of research on implicit theories of intelligence identified a finding whose application to health behaviour is direct and practically important. People who hold a fixed mindset — the belief that ability, talent, and capacity are largely innate and relatively unchangeable — respond to difficulty and setback in a fundamentally different way from people who hold a growth mindset, the belief that ability is developed through effort, learning, and persistence. The fixed mindset response to difficulty is typically withdrawal, avoidance, and a reduction in effort to protect the sense of capability from further threat. The growth mindset response is engagement, increased effort, and curiosity about what the difficulty reveals about what needs to be learned. (5)
Applied to health, the fixed mindset presents in several recognisable forms. The person who has tried and failed at a health programme before and concludes that they are not the kind of person who can sustain exercise. The person who believes their metabolism is categorically different from those of people who maintain healthy weight. The person who frames every difficulty in their programme as evidence of a fixed personal limitation rather than as information about what the programme or the approach needs to adjust. Each of these is a fixed mindset position that the neuroplasticity research directly contradicts.
Fixed Mindset vs Growth Mindset Applied to Health — What Each Position Produces in Eight Scenarios
| Health Context | Fixed Mindset Response (The brain cannot change) | Growth Mindset Response (The brain is being trained right now) |
|---|---|---|
| Programme difficulty | Training is this hard because I am not naturally athletic. This will always be this hard for me. Others find this easy because they are built differently. | Training is this hard because I am asking my nervous system to execute patterns it has not yet myelinated. It will get easier, not because I will stop improving, but because improvement will produce a new, harder challenge. |
| Early programme plateau | My body does not respond. I have hit my genetic ceiling. This approach is not working for someone with my biology. | I am in the early consolidation phase of neural adaptation. The plateau is the neurological equivalent of the foundation being laid before the building goes up. |
| Habit formation difficulty | I am just not a disciplined person. I have tried to build these habits before and cannot sustain them. This is how I am wired. | The habit I am trying to build has a sparse, newly forming neural pathway. Discipline is not the variable. Repetition is. I am building the pathway right now. |
| Returning after a break | I have lost everything I built. Starting again is humiliating proof that I cannot maintain progress. I am back to square one. | The neural pathways built during the previous period did not disappear. They weakened through disuse. They return to strength much faster than they were originally built, because the pathway exists and needs only reactivation. |
| Age and change capacity | I am too old to build new habits or change my relationship with food and exercise. This is who I am now. Change was possible earlier. | Adult neuroplasticity is well-established across the full lifespan. Older adults show different rates of pathway formation than younger ones, but the capacity for significant change is present throughout life. |
| Comparison to others' ease | Other people find this easy because they are naturally better suited to it. My difficulty is evidence of a fundamental biological disadvantage. | Other people find this easy because their neural pathways are more thoroughly myelinated through longer practice. My current difficulty is a function of where I am in the pathway-building process, not of who I am. |
| Response to coaching feedback | Feedback about what is not working feels like a verdict on capability. Defensive response. Difficulty integrating corrective information. | Coaching feedback is information about which part of the neural architecture needs more deliberate practice. It accelerates the pathway-building process. It is valuable data, not judgment. |
| Long-term identity | I will always struggle with this. My relationship with food and exercise is fixed by my personality and my history. | My current relationship with food and exercise is a product of the neural architecture built by my history. I am building new architecture right now. The relationship is changing. |
The growth mindset position is not optimism. It is accuracy. The neuroscience supports it. The fixed mindset position is not realism. It is a belief held in the absence of the neurological evidence that would contradict it.
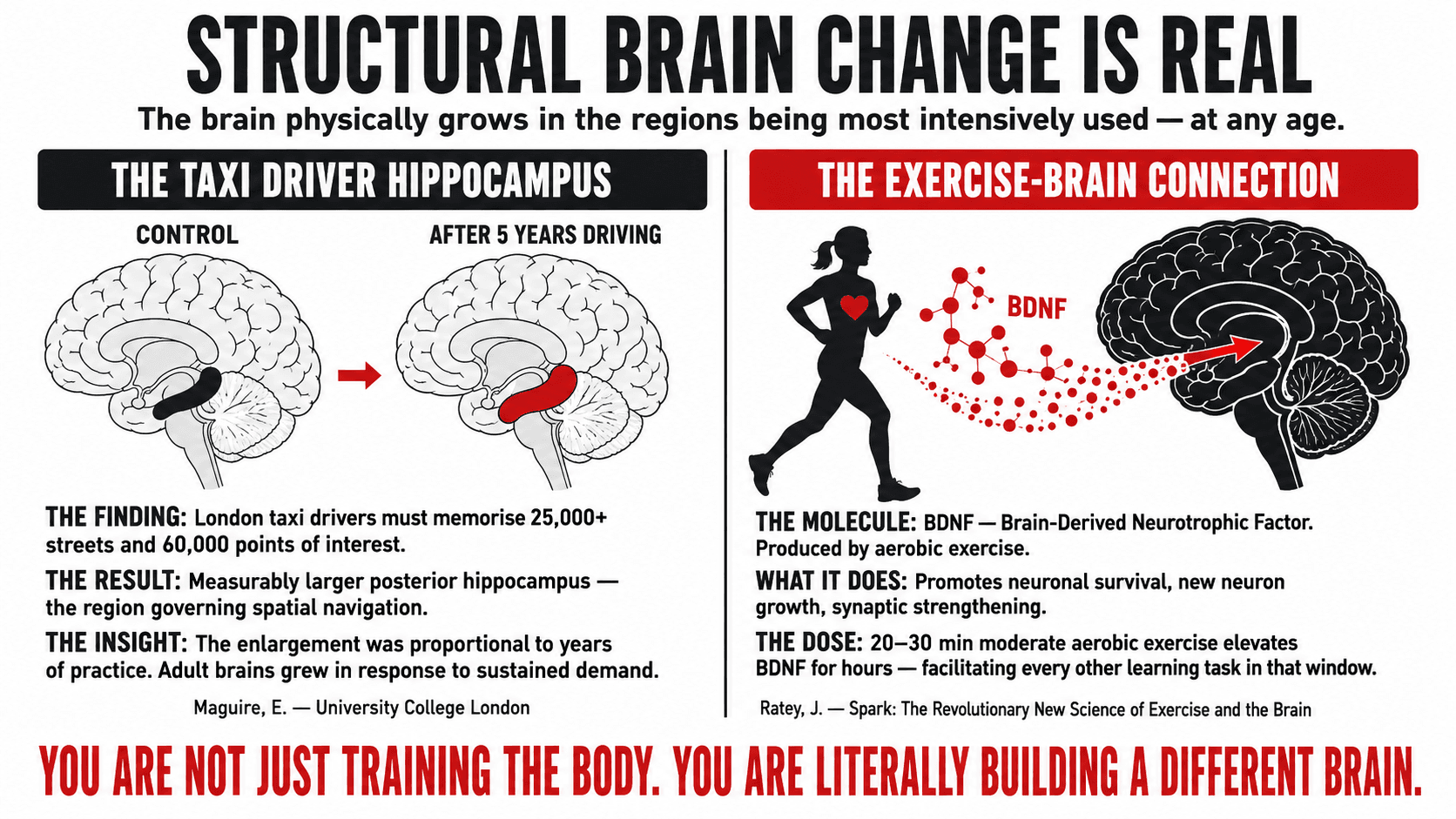
The Taxi Driver Hippocampus: What Structural Brain Change From Sustained Practice Looks Like
Eleanor Maguire's research at University College London provides one of the most compelling demonstrations of structural neuroplasticity in adult humans. London taxi drivers, who must memorise the layout of over twenty-five thousand streets and sixty thousand points of interest in order to pass the Knowledge examination, were found to have measurably larger posterior hippocampi than a matched control group — the posterior hippocampus being the region primarily responsible for spatial navigation and memory. The enlargement was proportional to the length of time the individual had been working as a taxi driver. The more years of navigation, the larger the hippocampal volume. The brain had physically grown in the region being most intensively used, in adult humans, in response to sustained practice. (6)
The practical implication for health behaviour change is not that health training produces visible brain enlargement, though exercise has been shown to increase hippocampal volume through a different mechanism involving BDNF, brain-derived neurotrophic factor. The implication is the demonstration of principle: sustained, consistent practice of a specific cognitive or physical demand produces structural changes in adult brain tissue that are measurable, that persist, and that are proportional to the extent of the practice. The person who practices consistent healthy behaviour is literally building a different brain from the one they currently inhabit. The process is invisible. The outcome is real.
John Ratey's research on exercise and the brain establishes the mechanism most directly relevant to health programme design. Aerobic exercise increases the production of BDNF, a protein that Ratey describes as Miracle-Gro for the brain: it promotes the survival of existing neurons, the growth of new ones, the strengthening of synaptic connections, and the general structural health of the brain tissue in regions including the hippocampus, the prefrontal cortex, and the cerebellum. Exercise is not simply a physical health intervention. It is a neurological one, producing structural brain changes that improve cognitive function, emotional regulation, stress resilience, and the very neural architecture that governs the habit formation and identity development processes described throughout this series. (7)
Key Insight: Every training session is doing two things simultaneously. It is producing the physical adaptations that the programme is designed to produce in muscle, cardiovascular capacity, and body composition. And it is producing the neurological adaptations that make the next session slightly more automatic, slightly less effortful, and slightly more congruent with the identity being built. The physical and the neurological improvements are inseparable. You cannot get one without the other. This is the case for consistent training that goes well beyond appearance.
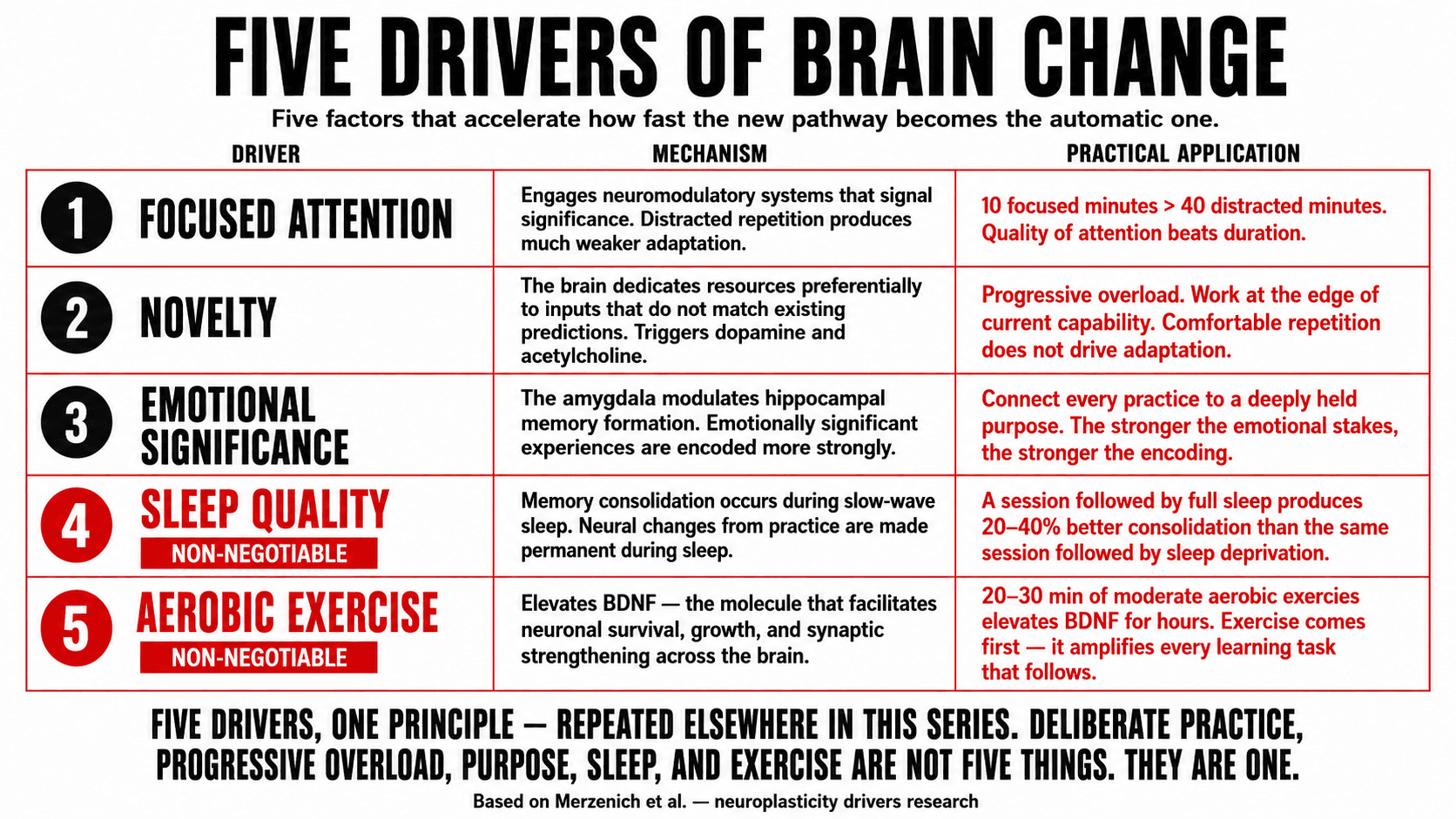
The Five Drivers of Neuroplasticity: What Accelerates Brain Change and What Blocks It
Neuroplasticity is not simply a passive response to repetition. Research from Merzenich and colleagues identified several factors that significantly modulate the rate and depth of neuroplastic change: the degree of focused attention during practice, the novelty of the experience, the emotional significance of the learning, the sleep quality following the practice session, and the aerobic exercise undertaken around the time of learning. Each of these factors can be deliberately managed to accelerate the pathway-building process, making the period of conscious effort before automation shorter and the quality of the resulting automated pattern higher. (1)
The Five Neuroplasticity Drivers — What Accelerates Brain Change in Each Health Domain
| Driver | The Mechanism | Health Application | Dose and Practical Notes |
|---|---|---|---|
| Focused attention | Neuroplastic change requires the engagement of the neuromodulatory systems that signal significance to the brain. Passive or distracted repetition produces much weaker pathway formation than attentive, deliberate practice. | Training performed with full attention to technique and sensation produces stronger motor pathway formation than the same training performed while distracted. Mindful eating builds the awareness pathway more efficiently than distracted eating. | Quality of attention during practice is more important than duration. Ten focused minutes of deliberate practice produces stronger neural adaptation than forty minutes of distracted repetition. This is Ericsson's deliberate practice finding applied neurologically. |
| Novelty | The brain dedicates neuroplastic resources preferentially to experiences that do not match existing predictions. Novel inputs trigger the release of acetylcholine and dopamine, creating optimal conditions for synaptic strengthening. | Progressive overload in training introduces novelty at the physiological level, maintaining the neurological conditions for adaptation. Nutritional variety prevents the eating pattern from becoming so automatic it bypasses conscious nutritional decision-making entirely. | The body of practice must remain at the edge of current capability to maintain novelty. Comfortable repetition within the mastered range does not trigger the same neuromodulatory response as practice at the boundary. |
| Emotional significance | Experiences with high emotional salience are encoded more strongly and recalled more readily than neutral ones. The amygdala modulates hippocampal memory formation, strengthening the encoding of emotionally significant experiences. | Health behaviour connected to a deeply valued personal purpose has higher emotional significance than the same behaviour executed as abstract self-improvement. The neurological encoding of the practice is stronger when the emotional stakes are genuine. | This is the neurological mechanism behind the mission-level goal architecture. The stronger the emotional connection to the purpose of the practice, the stronger the neural encoding of the practice itself. |
| Sleep quality | Memory consolidation and synaptic pruning occur primarily during slow-wave sleep. The neural changes produced during a learning or practice session are consolidated into long-term structural pathways during the subsequent sleep period. | A training session or new skill practice followed by adequate sleep produces stronger and more durable neural adaptation than the same session followed by insufficient sleep. Sleep is not merely recovery. It is the consolidation mechanism for the pathway being built. | Walker's research on sleep and learning suggests that a full night's sleep following a practice session can produce up to 20–40% improvement in recall and skill consolidation compared to sleep deprivation. The argument for sleep as part of every programme, not a peripheral consideration. |
| Aerobic exercise | Aerobic exercise increases BDNF production, which promotes neuronal survival, synaptic growth, and the general health of brain tissue in regions critical for learning and memory. It is both a neuroplasticity driver and a health behaviour. | Aerobic exercise performed before or immediately after a learning session or new habit practice has been shown to enhance the consolidation of the new material. Exercise is both the practice and the neurological facilitator of all other practice. | Ratey's research suggests that even twenty to thirty minutes of moderate aerobic exercise produces measurable BDNF elevation for several hours, during which period learning and habit consolidation are facilitated. The exercise comes first. |
Every element of this series converges in this table. Focused attention is deliberate practice. Novelty is progressive overload. Emotional significance is purpose-driven goal architecture. Sleep quality is the non-negotiable anchor. Aerobic exercise is the most important behaviour in the entire programme. These are not five separate considerations. They are five expressions of the same underlying principle.
The Return After Absence: Why Previous Training Is Never Truly Lost
One of the most practically important findings in neuroplasticity for anyone who has had a significant break from health behaviour is the phenomenon of muscle memory and the reactivation of established neural pathways. The popular concept of muscle memory refers to the fact that physical skills previously learned are reacquired far more rapidly after a break than they were originally acquired. The mechanism is neurological: the myelinated pathways built during the original practice period do not disappear when the practice stops. They weaken through disuse, the myelin sheath thinning and the synaptic connections reducing in strength, but the structural pathway remains encoded in the neural architecture. When practice resumes, the existing pathway is reactivated and remyelinated rather than built from scratch. (8)
The person returning to training after a period of absence is not starting from zero. They are starting from a weaker version of where they left off, with the neurological infrastructure of the previous period intact and ready for reactivation. The return to previous performance levels typically occurs in a fraction of the time required for the original development. This is why the person who trained seriously for five years and then stopped for two years returns to meaningful fitness in a few months, while the person who has never trained at all requires considerably longer to reach the same level.
The same principle applies to nutritional habits, sleep patterns, and cognitive frameworks. The person who established good nutritional habits for a sustained period, then deviated from them, is not re-learning from scratch. They are reactivating neural pathways that remain available, and the reactivation is typically faster, less effortful, and more stable than the original establishment. This is a significant source of encouragement for anyone who has previously built a period of good health behaviour: nothing from that period was wasted. The neural architecture built then is still there, waiting to be called back into active service.
Key Insight: If you have had a previous period of consistent training or healthy eating that you feel you have now lost, you have not lost it. You have allowed those pathways to weaken through disuse. The pathways exist. They need reactivation, not reconstruction. The return will feel harder than the maintenance did at its peak but significantly easier than the original establishment was. Expect to return to functional capability within four to eight weeks of consistent practice rather than the four to eight months the original establishment required.
Neuroplasticity in Practice: How the Brain Science Informs the Programme
The neuroplasticity research has specific practical implications for how I design programmes and how I frame the experience of the early and middle phases to clients. The single most important shift it produces is from a willpower narrative to a pathway-building narrative. The person struggling in weeks three to eight of a new health programme is not experiencing a failure of character or discipline. They are experiencing the expected difficulty of an unmyelinated pathway in the early stages of its formation. That reframe changes everything about how the difficulty is interpreted and whether the person stays through it.
The second implication is for the design of progressive overload in both training and nutritional practice. The brain's neuroplastic response is maintained by novelty and challenged by comfort. A programme that keeps the person working at the edge of their current capability is not simply a physical training principle. It is a neurological one. The training that feels slightly too hard is the training that is producing the most neurological adaptation. The training that feels comfortable and familiar is consolidating existing pathways, which has value, but is not building new ones.
The third implication is for the programme design around sleep and aerobic exercise, both of which function as neuroplasticity amplifiers rather than simply as health behaviours in their own right. The client who sleeps adequately is consolidating every session's neural adaptations more effectively than the client who does not. The client whose programme includes regular aerobic exercise is facilitating the formation of every other habit and skill in the programme through elevated BDNF. I work one-to-one with clients online globally. The programme I build is grounded in the neuroscience of how the brain actually changes.
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- Merzenich M. Soft-Wired: How the New Science of Brain Plasticity Can Change Your Life. San Francisco: Parnassus Publishing; 2013.
- Doidge N. The Brain That Changes Itself: Stories of Personal Triumph from the Frontiers of Brain Science. London: Penguin; 2007.
- Hebb DO. The Organisation of Behaviour: A Neuropsychological Theory. New York: Wiley; 1949.
- Fields RD. White matter in learning, cognition and psychiatric disorders. Trends in Neurosciences. 2008; 31(7): 361–370.
- Dweck CS. Mindset: The New Psychology of Success. New York: Random House; 2006.
- Maguire EA, Gadian DG, Johnsrude IS, et al. Navigation-related structural change in the hippocampi of taxi drivers. Proceedings of the National Academy of Sciences. 2000; 97(8): 4398–4403.
- Ratey JJ. Spark: The Revolutionary New Science of Exercise and the Brain. New York: Little, Brown; 2008.
- Staron RS, Leonardi MJ, Karapondo DL, et al. Strength and skeletal muscle adaptations in heavy-resistance-trained women after detraining and retraining. Journal of Applied Physiology. 1991; 70(2): 631–640.