
The Bone Density Clock Has Been Running Longer Than You Realise
Osteoporosis prevention for women is one of those health conversations that consistently arrives too late. Most women first hear about bone density when they are already post-menopausal, when a DEXA scan reveals a T-score that is lower than it should be, or when a fracture from a minor fall prompts an investigation that uncovers years of silent bone loss. By that point, the window for building peak bone density has closed. The interventions available are valuable but they are playing defence, not offence.
Bone density peaks in women in their late 20s. From that point, the trajectory is determined by the choices and circumstances of every decade that follows. The calcium intake in a woman's 30s. The resistance training in her 40s. The oestrogen levels that drop at menopause. The vitamin D status in every year from adolescence onward. The bone density that fractures a hip in a woman's 70s was shaped by the cumulative effect of decades of inputs that most women were never told were relevant.
This article is the guide I wish every woman received at 25. It explains what bone density is, how it is measured, how it is built and maintained, what threatens it, and what the evidence supports for protecting it across every decade of a woman's life. The tools are available. They are not complicated. And the earlier they are applied, the more powerful they are.
What Bone Density Is and Why It Matters
Bone is a living tissue. It is continuously remodelled through the activity of two cell types: osteoblasts, which build new bone, and osteoclasts, which resorb old bone. In healthy, young adult bone, these processes are in balance. Bone mineral density reflects the net result of this ongoing remodelling: the amount of mineral, primarily calcium and phosphorus, deposited in the bone matrix per unit of volume.
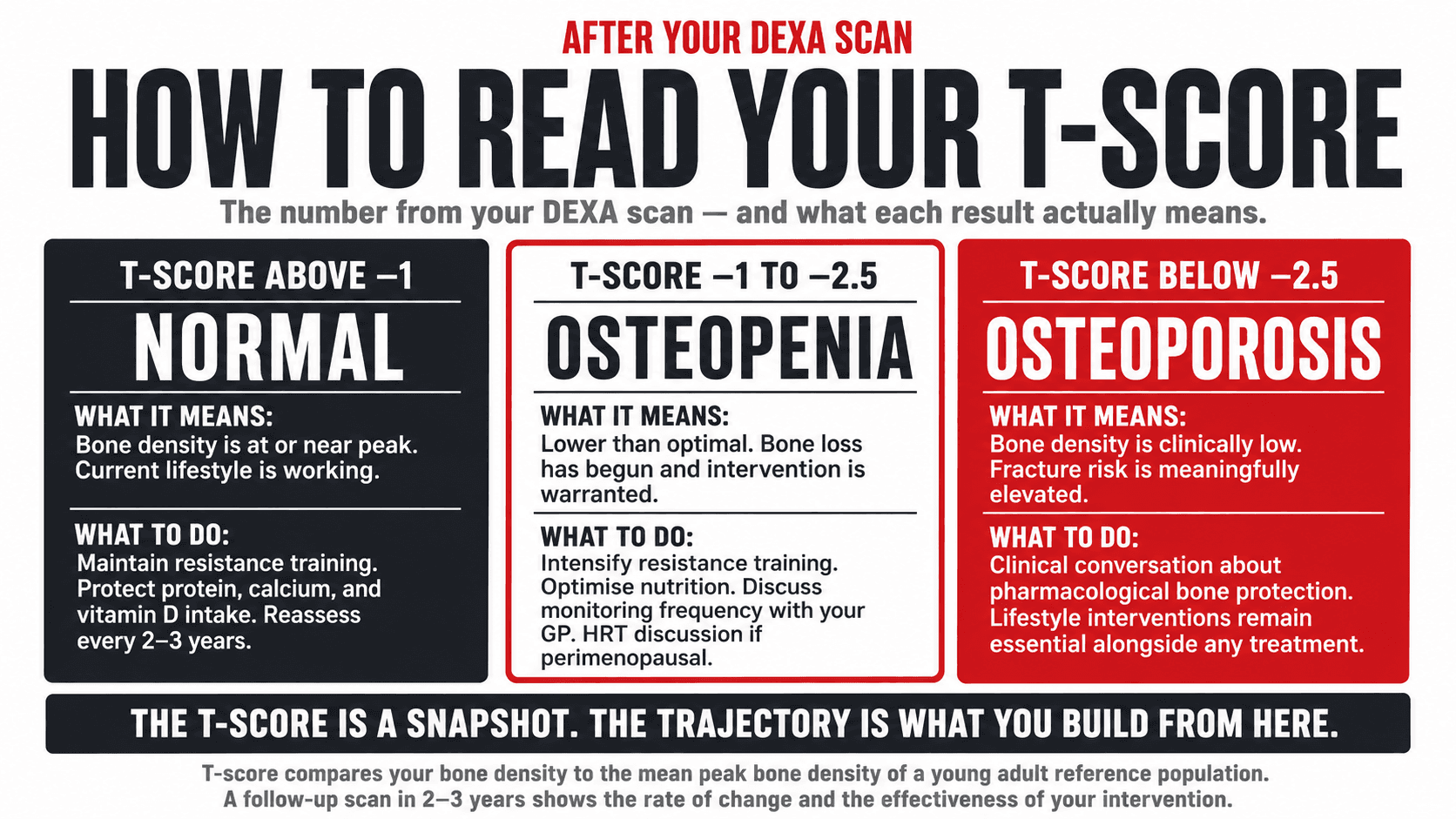
The clinical measurement of bone density is performed using a DEXA scan, dual-energy X-ray absorptiometry. The result is expressed as a T-score, which compares a woman's bone density to the mean peak bone density of a young adult reference population. A T-score above minus one is considered normal. Between minus one and minus two point five is classified as osteopenia, indicating lower than optimal bone density that warrants attention and intervention. Below minus two point five is classified as osteoporosis, the point at which fracture risk is clinically significant (1).
Fracture risk is the reason bone density matters clinically. Osteoporotic fractures, particularly at the hip, spine, and wrist, are not minor inconveniences. Hip fracture in older women is associated with a one-year mortality rate of approximately 20 to 30% and significant loss of independence in those who survive (2). Vertebral fractures cause chronic pain, loss of height, and postural changes that affect breathing, digestion, and quality of life. The fracture that happens at 75 is the consequence of bone density built or not built in the decades before. This is not theoretical. It is the biological reality that the bone density conversation needs to be grounded in.
Top Tip
Ask your GP for a DEXA scan if you are over 50, have gone through early menopause (before 45), have a family history of osteoporotic fracture, have taken corticosteroids for more than three months, have a history of an eating disorder, or have rheumatoid arthritis. In the UK, DEXA scans are available on the NHS via GP referral for women who meet clinical criteria. If you do not meet NHS criteria but want a baseline assessment, private scans cost approximately £80 to £150 and take less than thirty minutes.
The Bone Density Lifecycle in Women: When It Builds and When It Falls
Understanding where you are on the bone density curve is the most important context for understanding what interventions are most relevant to you right now. The trajectory is consistent across most women, though the rate of decline is significantly modified by lifestyle, hormonal history, and nutrition.
THE BONE DENSITY LIFECYCLE IN WOMEN
Building, Peak, and Decline
01
Teens to 20s
Building
Driver
Oestrogen, nutrition, loading.
Consequence
Depends on nutrition and loading.
Action
Maximise peak: resistance training, calcium, vitamin D.
02
Late 20s
Peak
Driver
Genetic ceiling reached.
Consequence
Sets the ceiling for life.
Action
Protect and maintain: keep training, protein, nutrients.
03
30s to Early 40s
Slow Decline
Driver
Oestrogen maintaining.
Consequence
Minor losses begin.
Action
Slow the decline: resistance training remains the key.
04
Perimenopause
Accelerating Loss
Driver
Oestrogen fluctuating and declining.
Consequence
Losses accelerate.
Action
Critical window: resistance training and HRT discussion.
05
Post-Menopause
2–3% Per Year Loss
Driver
Oestrogen withdrawn.
Consequence
Significant ongoing loss.
Action
Preserve and protect: training, nutrition, HRT if appropriate.
06
Later Decades
Cumulative Deficit
Driver
Accumulated loss.
Consequence
Osteoporosis and fracture risk.
Action
Maintain what remains: never stop loading.
The bone density you build by your late 20s is the ceiling you carry for life. Everything after that is about how slowly you lose it. The single most important variable at every stage is mechanical loading through resistance training.
How Resistance Training Builds Bone: The Mechanism Every Woman Should Understand
Bone responds to mechanical force. When force is applied to bone through muscle contraction and gravitational loading, the bone structure detects the stress and responds by stimulating osteoblast activity, building new bone tissue to meet the demand. This is the fundamental mechanism of exercise-induced bone formation, and it is the reason that resistance training is the most evidence-supported lifestyle intervention for bone density at every stage of life.
The loading must be sufficiently intense to stimulate the bone remodelling response. Low-load activities such as swimming and cycling, while excellent for cardiovascular health, do not generate the mechanical forces required to stimulate meaningful bone formation. Walking produces some benefit at the hip but minimal benefit at the spine. Running produces moderate benefit at specific sites but carries injury risk that limits its utility as a primary bone loading strategy. Resistance training with progressive loading, particularly with exercises that transmit force through the spine and hip, produces the most direct and site-specific bone density stimulus available through lifestyle alone (3).
The most clinically important sites for fracture risk in women are the femoral neck (hip), the lumbar spine, and the distal radius (wrist). Exercises that load these sites specifically produce the most relevant bone density improvements. Squats and deadlifts load the hip and lumbar spine under compression. Overhead press loads the thoracic and lumbar spine. Rows load the thoracic spine. Farmers' carries load the entire axial skeleton under gravitational force. These are not exotic exercises. They are the compound movements that form the foundation of any intelligent resistance training programme.
Research from the LIFTMOR trial demonstrated significant improvements in femoral neck and lumbar spine bone mineral density in postmenopausal women with osteopenia and osteoporosis following a programme of high-intensity progressive resistance and impact training, with no adverse skeletal events despite the high loading intensity (4). This finding is important because it challenges the instinct to protect fragile bones through rest and low-intensity exercise. The evidence suggests that appropriately supervised high-intensity loading is not only safe but more effective than low-intensity alternatives for post-menopausal bone health.
Top Tip
The four exercises that produce the most clinically relevant bone loading for women are the barbell or goblet squat, the conventional or Romanian deadlift, the overhead press, and the barbell row or farmer's carry. If your training programme does not include at least three of these four movements performed with progressive load, it is not adequately addressing your bone density. Add them. Progress them. Continue them throughout your life.

Bone Density Risk Factors for Women: What You Can and Cannot Change
| Risk Factor | Non-Modifiable | Modifiable |
|---|---|---|
| Genetics and family history | Family history of osteoporosis or hip fracture doubles personal risk. Genetic variants affect peak bone density ceiling and rate of decline. | Cannot change genetics, but the impact of genetic predisposition is substantially modified by lifestyle. A woman with a family history who trains and eats well will have meaningfully better bone health than one who does not. |
| Sex and age | Women lose bone faster than men post-menopause due to oestrogen withdrawal. Bone loss increases with age regardless of sex. | Cannot change sex or age. Can modify the rate of loss through every other variable on this table. The gradient is the variable, not the direction. |
| Hormonal status | Early menopause (before 45) significantly increases lifetime fracture risk due to longer period of oestrogen withdrawal. | HRT in eligible women meaningfully preserves bone density. Resistance training partially compensates for oestrogen withdrawal effect on bone. |
| Resistance training history | No non-modifiable component. | The single most modifiable risk factor. Progressive resistance training builds peak bone density in young women and preserves it in older women. Start at any age. Start now. |
| Calcium intake | No non-modifiable component. | Adequate calcium intake throughout life is essential for bone mineral deposition. Chronically low calcium accelerates bone loss. Dietary calcium first, supplementation to fill gaps. |
| Vitamin D status | No non-modifiable component. | Vitamin D is essential for calcium absorption. Deficiency, common in the UK, impairs both bone mineralisation and muscle function, increasing falls risk. Supplement year-round. |
| Protein intake | No non-modifiable component. | Protein provides the collagen matrix on which bone mineral is deposited. Adequate protein intake supports bone quality, not just quantity. This relationship is often overlooked in bone health discussions. |
| Smoking | No non-modifiable component. | Smoking is an independent risk factor for osteoporosis through direct effects on osteoblast function and through accelerating oestrogen metabolism. Cessation at any age reduces the ongoing damage. |
| Alcohol | No non-modifiable component. | Regular alcohol consumption suppresses osteoblast activity and impairs calcium absorption. More than two units per day consistently is associated with significantly increased fracture risk. |
| Body weight | No non-modifiable component. | Both very low body weight and significant excess body weight carry bone health risks. Low body weight reduces mechanical loading and oestrogen from adipose tissue. Excess body weight can impair mobility and increase fall consequence. Healthy body composition is the target. |
| Medications | Long-term corticosteroid use, certain anticonvulsants, aromatase inhibitors, and some SSRI antidepressants reduce bone density. | Discuss bone health monitoring and protective strategies with your GP if you use any long-term medications from these categories. Lifestyle measures remain important alongside any pharmacological bone protection. |
What the Absence of This Conversation Has Cost Women
Osteoporosis is sometimes described as a silent disease because it has no symptoms until a fracture occurs. This silence is compounded by a medical culture that has historically not prioritised bone density conversations with women until they are already in the post-menopausal years, by which point the window for building peak bone density has long closed and the intervention capacity is significantly reduced.
Approximately 3.5 million people in the UK have osteoporosis, and women account for the large majority of that figure, particularly in the post-menopausal population. One in two women over the age of 50 will experience an osteoporotic fracture in their lifetime (5). That is not a rare outcome. It is the statistical expectation for a population that has not been adequately informed or supported in building and maintaining bone health across the decades that determine the outcome.
The eating disorder population carries a disproportionate bone health burden that deserves specific mention. Women who have experienced restrictive eating disorders at any point in their lives, particularly in adolescence and early adulthood during the peak bone building window, often carry bone density deficits that persist decades later. The absence of adequate oestrogen and nutritional support during this critical period produces bone density losses that do not fully recover. If this applies to you, an early DEXA scan is a priority, not a routine screening for later life.
The perimenopausal years represent the last meaningful opportunity to influence the bone density trajectory before the oestrogen-withdrawal-driven acceleration of loss begins. Women who enter the perimenopausal transition having built strong bone density reserves through years of resistance training and adequate nutrition are in a fundamentally different position than those who have not. The difference is not subtle. It is the difference between a T-score that warrants monitoring and one that warrants urgent intervention.
Top Tip
If you have a history of an eating disorder, particularly one that involved restrictive eating during adolescence or your 20s, discuss this explicitly with your GP and ask for a baseline DEXA scan regardless of your age. The bone density deficit associated with this history is real, clinically significant, and worth knowing about so that targeted intervention can be prioritised now rather than discovered through a fracture later.
Nutrition for Bone Health: The Three Non-Negotiables and the One Most Women Miss
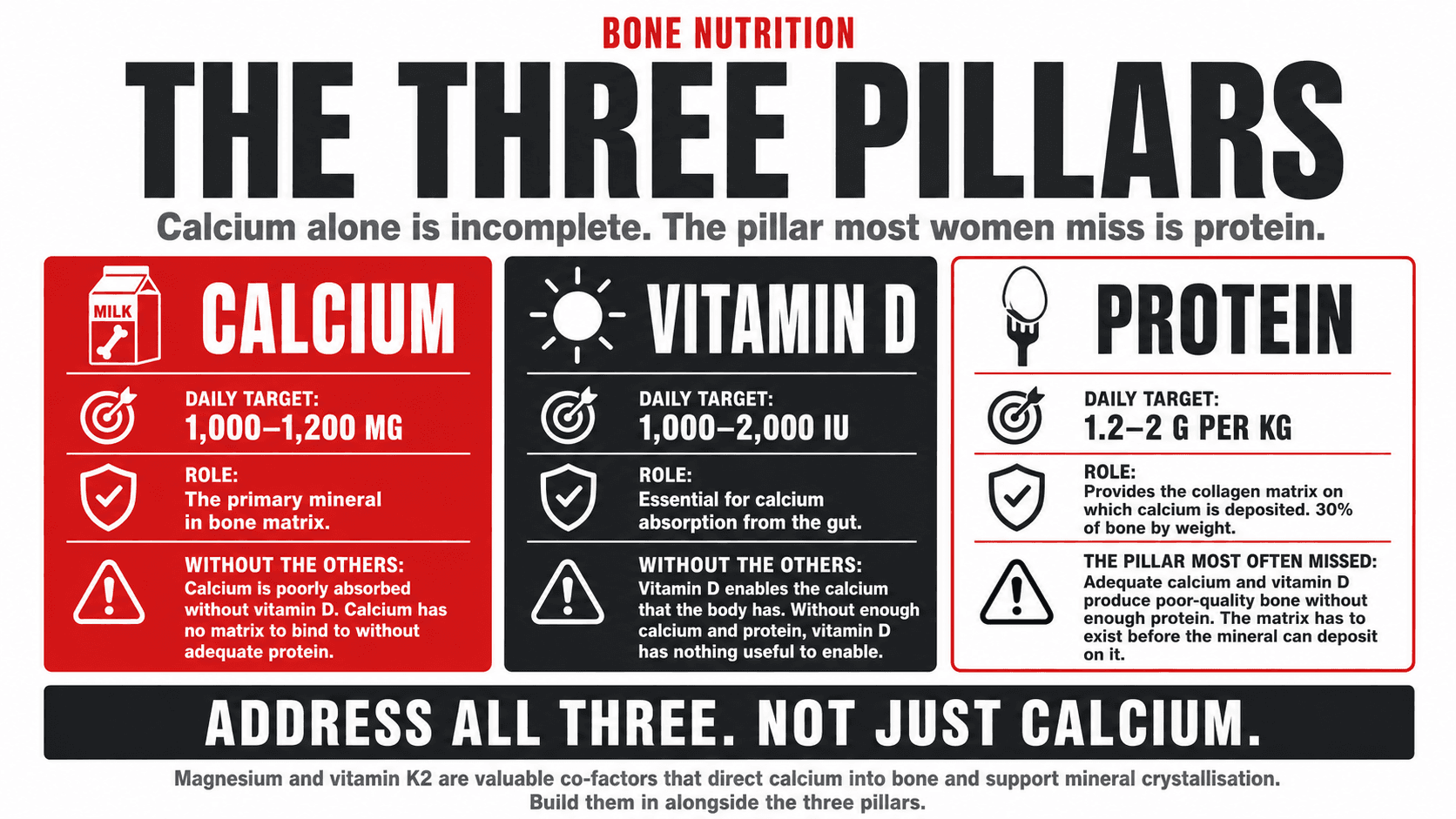
The nutritional side of bone health is frequently reduced to a single message: eat more calcium. That message is not wrong, but it is incomplete in ways that matter. The three primary nutrients for bone health are calcium, vitamin D, and protein. And the one that most women miss is protein.
| Nutrient | Daily Target | Role in Bone Health | Best Plant-Based Sources | Best Omnivore Sources |
|---|---|---|---|---|
| Calcium | 700mg (UK RNI). 1,000 to 1,200mg recommended post-menopause | Primary mineral in bone matrix. Essential for bone mineralisation and density maintenance. | Fortified oat, soy, or almond milk (120 to 300mg per 200ml). Calcium-set tofu (350mg per 100g). Kale (150mg per 100g). Broccoli. White beans. Sesame seeds and tahini. Almonds. | Dairy: milk, yoghurt, cheese (high bioavailability). Sardines with bones. Fortified plant milks. Same plant sources apply. |
| Vitamin D | 400IU minimum (UK PHE). 1,000 to 2,000IU recommended for bone health in most women | Essential for calcium absorption from the gut. Without adequate vitamin D, dietary calcium cannot be effectively utilised. | Sunlight (April to September in UK only). Fortified plant milks. Some mushrooms (UV-exposed). Supplementation is essential for most women year-round in the UK. | Oily fish (salmon, mackerel, sardines). Eggs. Fortified foods. UK sunlight insufficient year-round. Supplement regardless of diet. |
| Protein | 1.2 to 1.6g per kg per day minimum for bone health. 1.6 to 2g if training | Provides the collagen matrix (osteoid) on which calcium is deposited. Chronically low protein produces low-quality bone regardless of calcium intake. | Tofu, tempeh, soy protein, pea protein, lentils, chickpeas, black beans, edamame, quinoa, seitan. Spread across 3 to 4 meals. | Meat, fish, eggs, dairy, in addition to all plant sources. Variety supports comprehensive amino acid profile for collagen synthesis. |
| Magnesium | 270mg per day (UK RNI) | Co-factor for vitamin D activation and bone mineral crystallisation. Deficiency impairs bone quality. | Dark chocolate, pumpkin seeds, almonds, cashews, spinach, black beans, avocado, brown rice, quinoa. | Same plant sources are richest. Also found in whole grains and some seafood. |
| Vitamin K2 | No UK RNI. Emerging evidence suggests 100 to 200mcg per day is beneficial for bone | Activates osteocalcin, the protein that binds calcium into bone matrix. Directs calcium to bone rather than arterial walls. | Natto (fermented soy, very high). Sauerkraut, kimchi, miso (moderate). Small amounts in dark leafy greens. Supplementation often necessary. | Natto remains the richest source regardless of diet. Hard cheeses, egg yolk, liver. K2 supplementation as MK-7 form is practical for most. |
Calcium without adequate vitamin D is poorly absorbed. Vitamin D without adequate protein produces calcium that has nowhere to be properly deposited. All three nutrients are required together. Address all three, not just calcium alone.
The protein-bone connection is the most consistently overlooked element of bone nutrition. Bone is not purely mineral. Approximately 30% of bone by weight is the organic protein matrix, primarily collagen type 1, on which calcium phosphate crystals are deposited. Chronically low protein intake impairs collagen synthesis, produces lower-quality bone matrix, and reduces the structural integrity of bone independently of the mineral content measured on a DEXA scan. Women who eat adequate calcium but chronically undereat protein may have bone density numbers that look acceptable on a scan while carrying bone that is more brittle and more fracture-prone than the density figure suggests (6).
Top Tip
Check the label on the plant milk you use daily. Not all plant milks are fortified with calcium, and among those that are, the amount varies significantly. Look for at least 120mg of calcium per 100ml, which means approximately 240mg per standard 200ml glass. Oat milk, soy milk, and almond milk are all available in fortified versions. Shake the carton before use as the calcium can settle. A fortified plant milk used daily across three portions contributes meaningfully toward your calcium target without supplements.
Smoking, Alcohol, and Medications: The Bone Density Factors Nobody Talks About
Two lifestyle behaviours that significantly impair bone health and that do not receive adequate attention in bone health conversations deserve specific mention.
Smoking is an independent risk factor for osteoporosis and fracture. Nicotine directly impairs osteoblast function, reducing new bone formation. Smoking also accelerates the metabolism of oestrogen, effectively reducing the protective effect of endogenous oestrogen on bone during the premenopausal years. Women who smoke have lower peak bone density, faster rates of bone loss, and significantly higher fracture risk than non-smoking women of the same age and hormonal status (7). This is not a marginal effect. It is clinically meaningful at every stage of the bone density lifecycle.
Alcohol at more than two units per day consistently suppresses osteoblast activity, impairs calcium absorption in the gut, increases calcium excretion through the kidneys, and disrupts the liver metabolism of vitamin D. The cumulative effect on bone density is substantial. Women who drink regularly above the recommended limits carry meaningfully lower bone density for their age than those who do not, independent of other lifestyle factors (8). Reducing alcohol intake is not only a bone health intervention. It is a hormonal, metabolic, and sleep quality intervention simultaneously, all of which further support bone health indirectly.
Long-term corticosteroid use, which includes prednisolone taken for conditions including asthma, inflammatory bowel disease, and rheumatoid arthritis, is one of the most significant medication-related causes of bone loss. If you have been on corticosteroids for more than three months, a bone density assessment and a conversation with your GP about bone protection are both warranted and in many cases clinically indicated. This should be raised proactively rather than waited for.
Top Tip
If you smoke and are concerned about your bone health, stopping smoking is the single most impactful change you can make for your long-term fracture risk, second only to starting resistance training. The bone density damage from smoking is partially reversible after cessation, with the rate of further loss slowing toward that of a non-smoker over several years. There is no point in the lifecycle at which stopping smoking is not worthwhile for bone health.

When to Get a DEXA Scan and What to Do With the Results
DEXA scanning is the definitive method for assessing bone density and provides results that are specific, actionable, and directly relevant to treatment and lifestyle decisions. The question is not whether DEXA scanning is useful, it clearly is, but when it is appropriate to request one.
In the UK, NHS DEXA scanning is available via GP referral for women who meet clinical criteria assessed using the FRAX fracture risk assessment tool or who have specific risk factors including early menopause, long-term corticosteroid use, a history of fragility fracture, low BMI, or conditions associated with secondary osteoporosis. If you do not meet current NHS referral criteria but have personal risk factors or concerns, private DEXA scanning is widely available at a cost of approximately £80 to £150 and provides the same clinical information.
What to do with the results depends on the T-score. A normal T-score above minus one means the current lifestyle approach is working and should be maintained. Osteopenia between minus one and minus two point five warrants the lifestyle interventions described throughout this article, applied with greater intention and consistency, and a discussion with your GP about monitoring frequency and whether any additional support is appropriate. A T-score below minus two point five indicating osteoporosis warrants a clinical conversation about pharmacological bone protection alongside lifestyle intervention, and should be managed in partnership with your GP or a metabolic bone specialist.
Top Tip
Request a DEXA scan at around age 50 as a proactive baseline, regardless of whether you have visible risk factors. The result tells you your starting position for the post-menopausal years before they arrive, and it gives you a clear and specific target to work toward. A follow-up scan two to three years later shows the rate of change and the effectiveness of your intervention. You cannot manage what you cannot measure.
How Bone Health Is Built Into Every Programme I Write
Bone density is not an optional consideration that I address only with older clients. It is a structural element of the programme I build for every female client from the earliest conversation onward. The compound movements that form the foundation of every programme, squats, deadlifts, rows, presses, and carries, are not chosen arbitrarily. They are chosen because they load the axial skeleton and appendicular skeleton in the ways that the evidence supports for building and preserving bone at every stage of a woman's life.
The nutritional framework I build alongside training always addresses calcium, vitamin D, and protein in the context of bone health, not just body composition. These nutrients are not supplementary. They are foundational. A training programme without adequate nutritional support for bone mineralisation is leaving a significant proportion of its potential benefit unrealised.
If you are concerned about your bone density, have risk factors for osteoporosis, or simply want to build the strongest possible foundation for the decades ahead, I work one-to-one with women online globally. Bone health is one of the most important and most rewarding areas of women's health to address proactively. The work you do now pays dividends for the rest of your life. Let us build that foundation together.
