Alcohol and men's health are deeply intertwined in British culture. Drinks after work, beers at the game, wine with dinner, rounds at the pub, bottles at celebrations, nightcaps at home. For many men, drinking is so woven into the fabric of daily and social life that questioning it feels unnecessary, if not mildly offensive.
But the physiology does not care about cultural norms. Alcohol is a toxin. It is the only macronutrient that your body prioritises clearing above all else, to the temporary exclusion of fat burning, muscle building, and hormonal regulation. It is a Group 1 carcinogen classified by the World Health Organization. And it is, for a large number of men I work with, the single biggest unacknowledged barrier to the results they say they want.
This article is not about abstinence. It is about honesty. About what the evidence actually shows, so that you can make a properly informed decision about your relationship with alcohol and what, if anything, you want to do about it.
The Conversation Nobody in the Fitness Industry Wants to Have
Personal trainers and fitness coaches often avoid the alcohol conversation. It is uncomfortable. Clients push back. People feel judged. And in an industry that is heavily reliant on client retention and referrals, telling someone that their Friday night drinking habit is undermining their results is not always commercially popular.
I have chosen to have the conversation anyway, because my job is to give clients the information they need to make real progress, not the information they find easiest to hear. Alcohol is not compatible with optimal body composition, hormonal health, sleep quality, or cancer risk reduction. That does not mean it has to be eliminated. It means it needs to be understood and accounted for honestly.
How Your Body Processes Alcohol: The Basics
When you consume alcohol, it is absorbed rapidly from the stomach and small intestine into the bloodstream. The liver becomes the primary site of metabolism, converting ethanol to acetaldehyde via the enzyme alcohol dehydrogenase, and then to acetate via aldehyde dehydrogenase.
The key point is this: acetaldehyde is toxic. It is the compound primarily responsible for cellular damage associated with chronic alcohol consumption. The liver processes it as quickly as possible, but that process takes priority over virtually every other metabolic function.
While alcohol is present in the bloodstream, fat oxidation is substantially reduced. The liver is too busy clearing ethanol to carry out lipid metabolism at normal rates. Alcohol itself provides 7 kilocalories per gram, making it the second most energy-dense macronutrient after fat, but unlike fat, protein, or carbohydrate, it has no structural or functional role in the body whatsoever.
Top Tip
Alcohol does not just add calories. It changes the metabolic environment your body operates in for the hours it takes to clear it. During that window, fat burning largely stops, anabolic hormone secretion is impaired, and your body is in a fundamentally different physiological state from the one you are trying to cultivate with your training and nutrition.

Alcohol and Testosterone: The Hormonal Mechanism
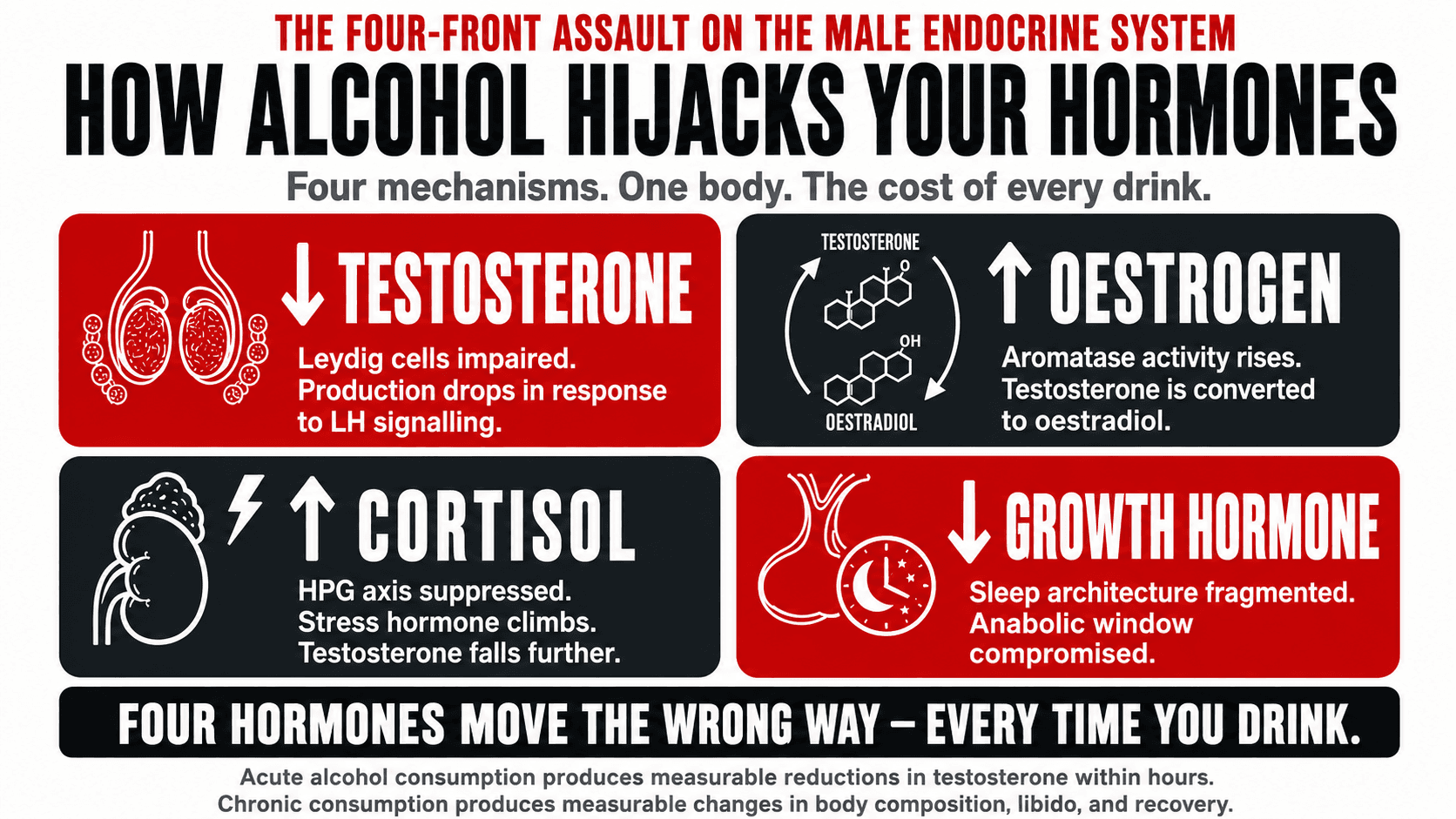
Testosterone is produced primarily in the Leydig cells of the testes. These cells are sensitive to ethanol. Alcohol directly impairs Leydig cell function, reducing their ability to produce testosterone in response to luteinising hormone (LH) signalling from the pituitary gland (1).
Simultaneously, alcohol elevates the activity of aromatase, the enzyme responsible for converting testosterone to oestradiol. This creates a dual mechanism: less testosterone is produced, and a greater proportion of what is produced is converted to oestrogen. The result is a reduced testosterone-to-oestrogen ratio that, when repeated regularly, can produce meaningful hormonal disruption.
Alcohol also elevates cortisol. Cortisol and testosterone have an inverse relationship. As cortisol rises, the hypothalamic-pituitary-gonadal axis is suppressed, further reducing testosterone output. This is not a subtle or theoretical effect. Acute alcohol consumption produces measurable reductions in testosterone within hours (2).
In men who drink regularly, chronic testosterone suppression contributes to reduced muscle mass, increased body fat, reduced libido, impaired erectile function, low energy, reduced motivation, and mood disturbance. Many of these symptoms are attributed to stress, ageing, or overtraining, when the primary driver is sitting in the fridge.
Top Tip
If you are experiencing unexplained fatigue, reduced motivation, difficulty building or maintaining muscle, low libido, or mood changes, and you drink alcohol regularly, the alcohol is a plausible contributing factor that deserves honest consideration before you investigate more complicated explanations.
How Alcohol Disrupts the Male Hormonal System
The hormonal disruption caused by regular alcohol consumption is not confined to testosterone alone. Alcohol affects the entire hypothalamic-pituitary-gonadal axis, suppresses growth hormone secretion, dysregulates insulin and glucagon, and alters thyroid hormone conversion. It is a systemic endocrine disruptor, not a single-hormone issue.
Alcohol and Sleep: Why Passing Out Is Not the Same as Sleeping
Many men report that alcohol helps them sleep. It is true that alcohol has a sedative effect and can shorten the time it takes to fall asleep. But sedation is not sleep. The sleep architecture produced after alcohol consumption is profoundly abnormal.
In the first half of the night, alcohol suppresses REM sleep and can increase slow-wave sleep in some individuals. This creates a false impression of deep, restful sleep. But as blood alcohol levels fall in the second half of the night, the brain undergoes a rebound into a heightened state of arousal. This produces REM rebound, micro-arousals, lighter and more fragmented sleep, and often early waking.
The consequences for men are significant. Growth hormone is predominantly secreted during deep sleep in the first half of the night. REM sleep in the second half of the night is when testosterone secretion is consolidated. When alcohol fragments this architecture, both hormones are compromised in a single night.
Top Tip
If you drink in the evenings regularly and wake feeling unrested, wake in the early hours, or feel groggy despite adequate hours in bed, the alcohol is very likely the primary cause. The sedative effect fools you into thinking you slept well. The fragmented second half of the night quietly undermines your hormonal recovery, muscle repair, and cognitive restoration — leaving you in an accumulating sleep debt you may not even recognise.
What One Night of Drinking Does to Your Body
| Timeframe | What Is Happening in Your Body |
|---|---|
| 0 to 1 hour | Alcohol enters the bloodstream. The liver begins prioritising alcohol metabolism above all else. Fat oxidation stops. Blood glucose rises initially then may fall as insulin is released in response to the caloric load. |
| 1 to 3 hours | Blood alcohol is at or near its peak. Leydig cells are impaired. Testosterone production is already being suppressed. Aromatase activity is elevated. Cortisol is rising. If consuming multiple drinks, this phase extends and deepens. |
| 3 to 6 hours | Blood alcohol is clearing. As it falls, the brain begins a rebound into alertness. Sleep architecture starts to fragment. Deep slow-wave sleep is disrupted. The individual may be unconscious but they are not sleeping in any physiologically meaningful sense. |
| 6 to 8 hours | If asleep, the rebound phase is active. Micro-arousals are occurring. Growth hormone pulse amplitude is reduced. Testosterone secretion during REM is impaired. The body has now spent several hours in a disrupted hormonal state during what should have been its most anabolic window. |
| Next morning | Cortisol is elevated. Testosterone is below its rested baseline. Ghrelin is up and leptin is down, producing stronger appetite and cravings. Dehydration impairs cognitive function and perceived energy. Inflammation markers are elevated. Muscle protein synthesis is impaired. |

The Calorie Cost of Alcohol
Beyond the hormonal and sleep disruption, alcohol carries a direct caloric cost that most men significantly underestimate. At 7 kilocalories per gram, a standard evening of drinking can easily represent 500 to 1,000 or more calories that are invisible in most food tracking approaches because they are not food.
The table below illustrates the energy cost of common drinks alongside a practical comparison to help contextualise the numbers.
| Drink | Standard Units | Approximate Calories | Equivalent Walk |
|---|---|---|---|
| Pint of lager (5%) | 2.3 units | 210 to 230 kcal | 40 to 50 minutes |
| Large glass of wine (250ml, 13%) | 3.3 units | 210 to 230 kcal | 40 to 50 minutes |
| Double gin and tonic | 2.0 units | 150 to 170 kcal | 30 to 35 minutes |
| Cocktail (e.g. Mojito or Espresso Martini) | 2.0 to 3.0 units | 200 to 280 kcal | 40 to 55 minutes |
| 4 pints on a Saturday night out | 9.2 units | 840 to 920 kcal | Nearly 3 hours |
| Non-alcoholic lager (e.g. Heineken 0.0) | 0.0 units | 21 kcal per 330ml | Under 5 minutes |
| Non-alcoholic spirit and tonic | 0.0 units | Under 50 kcal | Under 10 minutes |
These numbers do not include the food typically consumed alongside drinking, which research consistently shows is greater in volume, higher in calorie density, and less nutritionally optimal when alcohol is present. Alcohol impairs the prefrontal cortex activity responsible for impulse control and decision-making, making the late-night kebab or the second helping of chips significantly more likely.
The Group 1 Carcinogen Most Men Have Never Considered
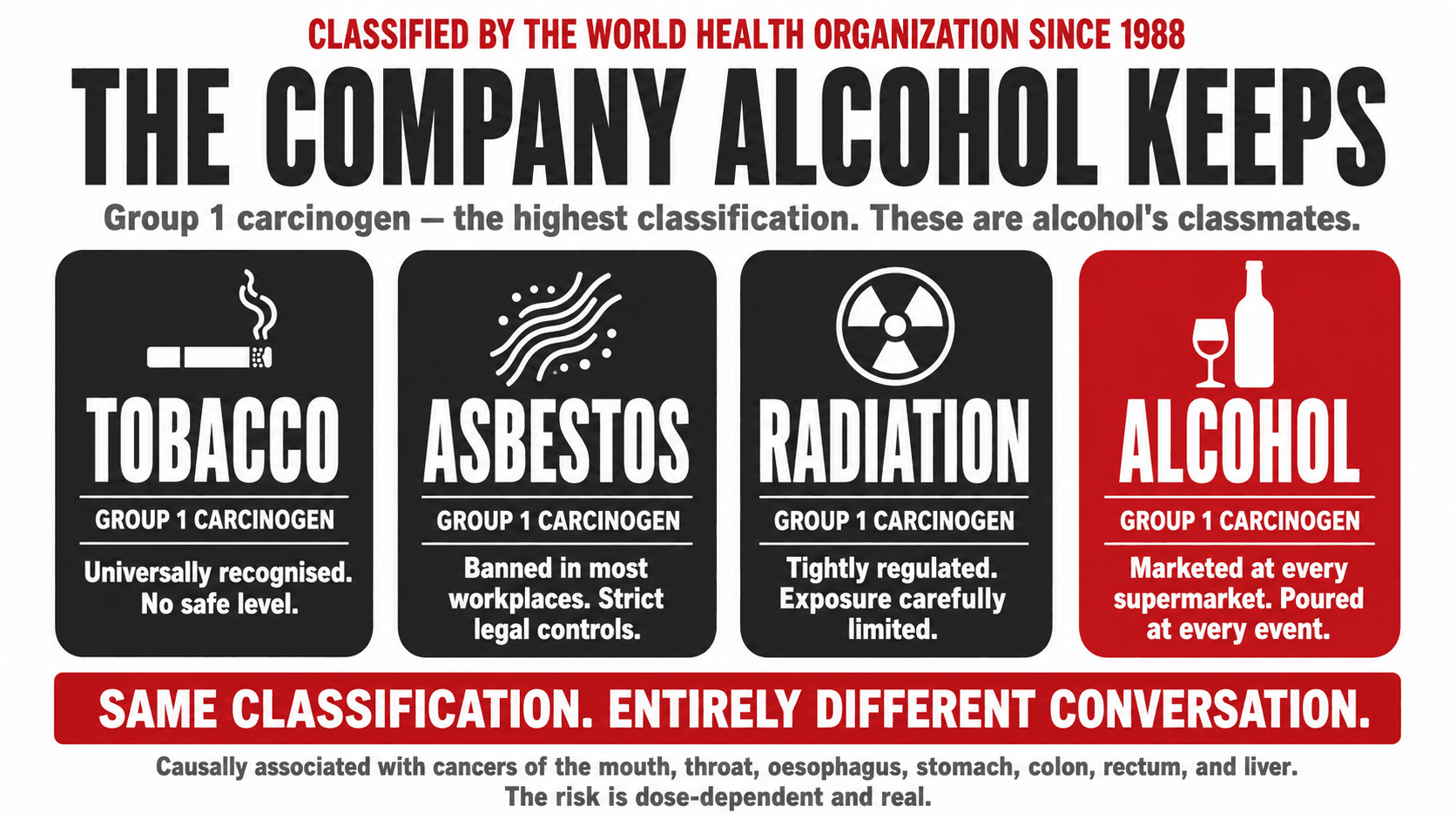
In 1988, the International Agency for Research on Cancer classified alcohol as a Group 1 carcinogen. This is the highest classification, meaning there is sufficient evidence that alcohol causes cancer in humans. It shares this classification with tobacco smoke, asbestos, and radiation.
Alcohol is causally associated with cancers of the oral cavity, pharynx, larynx, oesophagus, stomach, colon, rectum, and liver. There is also evidence of an association with breast cancer in women and emerging evidence for prostate cancer in men (5). These are not marginal associations. They are dose-dependent relationships, meaning risk increases with the amount consumed.
Most men who drink regularly are entirely unaware of this classification. The messaging around moderate alcohol consumption in the media has historically been dominated by stories about cardiovascular benefit from red wine, a narrative that has been substantially revised in recent years as more rigorous study designs have been applied and confounding variables have been better controlled for (6).
The current scientific consensus, reflected in updated WHO and NHS guidance, is that no level of alcohol consumption is entirely risk-free when it comes to cancer. This does not mean a single drink at Christmas will give you cancer. It means that the risk is real, dose-dependent, and worth understanding as part of an informed decision about how you choose to live.
The Moderate Drinking Myth: What the Research Actually Shows
For several decades, observational studies suggested that moderate drinkers had lower cardiovascular mortality than non-drinkers. This finding was widely reported and contributed to the cultural normalisation of alcohol as part of a healthy lifestyle.
The problem is that many of these studies were methodologically flawed. The non-drinking group included sick quitters, people who had stopped drinking due to illness, and lifelong abstainers who may have had other health vulnerabilities. When these confounding factors are properly controlled for, the apparent protective effect of moderate alcohol largely disappears (7).
Mendelian randomisation studies, which use genetic variants as natural experiments to test causal relationships, have found no evidence of a protective effect of moderate alcohol consumption on cardiovascular outcomes when genetic confounders are accounted for (8). The moderate drinking benefit appears to have been largely a statistical artefact rather than a genuine biological mechanism.
Practical Strategies for Reducing Alcohol Without Losing Your Social Life
Recommending that men simply drink less is not a strategy. It is a platitude. What actually works is addressing the specific situations, habits, and social dynamics that drive drinking, and providing practical alternatives that do not require social isolation or constant willpower.
Know your weekly unit total. Most men have no accurate idea how much they actually drink. Tracking for one week without changing anything, using a unit calculator, typically produces a number that surprises people.
Set a weekly unit budget. The NHS recommends no more than 14 units per week and advises spreading them across at least three days. Treating this as a real budget with a weekly total changes the decision-making framework from moment-to-moment willpower to advance planning.
Designate alcohol-free days. Not as punishment, but as a structural tool. When certain days are simply off the table, the decision does not need to be made repeatedly. Two to three alcohol-free days per week creates meaningful reduction in weekly totals without requiring any single evening of white-knuckling.
Use the no-alcohol category. The quality of non-alcoholic beer, wine, spirits, and mixers has improved dramatically. Brands like Heineken 0.0, Guinness 0.0, Seedlip, and Lyre's provide options that satisfy the social ritual of drinking without the physiological consequences. In a pub environment, a non-alcoholic beer in a pint glass looks identical to the real thing.
Shift the framing. Reducing alcohol is not giving something up. It is recovering testosterone, sleep quality, body composition, cognitive function, and cancer risk reduction. Framed as addition rather than restriction, it becomes considerably easier to sustain.
Top Tip
Start by tracking your units honestly for one week without changing anything. Do not estimate. Use an online unit calculator and record every drink. Most men find that this single exercise produces an accurate picture of their intake that differs significantly from their self-assessment, and that awareness alone begins to shift behaviour.

My Approach With Clients Who Drink
I do not require clients to stop drinking. I do require them to be honest about how much they drink, to understand the physiological consequences, and to make a conscious decision about whether their current alcohol intake is consistent with the goals they say they have.
For most men, once they have the information laid out clearly and honestly, they choose to reduce. Not because I told them to, but because they can see plainly that what they are doing is working against what they want. The hormonal disruption is real. The sleep disruption is real. The caloric cost is real. The cancer risk is real.
What I have also seen, repeatedly, is the positive change that comes from meaningful reduction. Clients who cut from four nights a week of drinking to one, or from eight units a week to three, typically report better sleep within the first week, improved energy within two, and measurable changes in body composition, mood, and training performance within a month. These are not dramatic interventions. They are modest reductions in a single variable that was carrying an outsized physiological cost.
You do not have to be teetotal to be healthy. But you do need to be honest. If your training is consistent, your nutrition is solid, and your progress has stalled, the question I would ask you is the same one I ask every client who has not asked it of themselves: how much are you drinking, and is that number consistent with the results you want?
Work with Me
Get a personalised coaching plan built around your goals, your schedule, and your life.
Enquire NowReferences
- (1) Emanuele MA, Emanuele NV. Alcohol's effects on male reproduction. Alcohol Health Res World. 1998;22(3):195-201.
- (2) Sierksma A, Sarkola T, Eriksson CJ, et al. Effect of moderate alcohol consumption on plasma dehydroepiandrosterone sulfate, testosterone, and estradiol levels in middle-aged men and postmenopausal women. Alcohol Clin Exp Res. 2004;28(5):780-785.
- (3) Rachdaoui N, Sarkar DK. Effects of alcohol on the endocrine system. Endocrinol Metab Clin North Am. 2013;42(3):593-615.
- (4) Colrain IM, Nicholas CL, Baker FC. Alcohol and the sleeping brain. Handb Clin Neurol. 2014;125:415-431.
- (5) World Health Organization. Alcohol. WHO Fact Sheet. Geneva: WHO; updated 2023.
- (6) Burton R, Sheron N. No level of alcohol consumption improves health. Lancet. 2018;392(10152):987-988.
- (7) Holmes MV, Dale CE, Zuccolo L, et al. Association between alcohol and cardiovascular disease: Mendelian randomisation analysis based on individual participant data. BMJ. 2014;349:g4164.
- (8) Millwood IY, Walters RG, Mei XW, et al. Conventional and genetic evidence on alcohol and vascular disease aetiology: a prospective study of 500,000 men and women in China. Lancet. 2019;393(10183):1831-1842.
- (9) Bendtsen P, Johansson K, Akerlind I. Feasibility of an email-based electronic screening and brief intervention (e-SBI) to reduce risky drinking among university students. Subst Abuse Treat Prev Policy. 2006;1:32.
- (10) Rao R, Topiwala A. Alcohol use disorders and the brain. Addiction. 2020;115(8):1580-1589.
- (11) NHS. Alcohol units. National Health Service; updated 2022. Available at: nhs.uk/live-well/alcohol-advice/calculating-alcohol-units
- (12) Traversy G, Chaput JP. Alcohol consumption and obesity: an update. Curr Obes Rep. 2015;4(1):122-130.